If you have IJV compression, you will need surgery to allow your IJVs to reopen so normal blood flow can occur out of your brain. The doctor who said what your scans show is normal is clearly not familiar w/ what normal anatomy looks like in that part of your neck. An IJV should never have an area that is “flat”.
Extremely thick & long styloids sounds pretty awful. We will be interested in seeing your scans if you’re able to make 3D renderings of them. If you Google CT scan 3D slicer software, links for some you can use free of charge will come up. A number of our members here have created their own 3D images, so if you get stuck, send out an SOS, & I’m sure someone (not me, not computer savvy here ) will com to your rescue from our forum.
Like Isaiah said, no, jugular veins shouldn’t appear collapsed or stenosed on scans. If that were the case, what’s the point of a scan?
Unfortunately it does not seem that Dr is familiar at all with this condition. Furthermore, your styloids are clearly calcified and elongated.
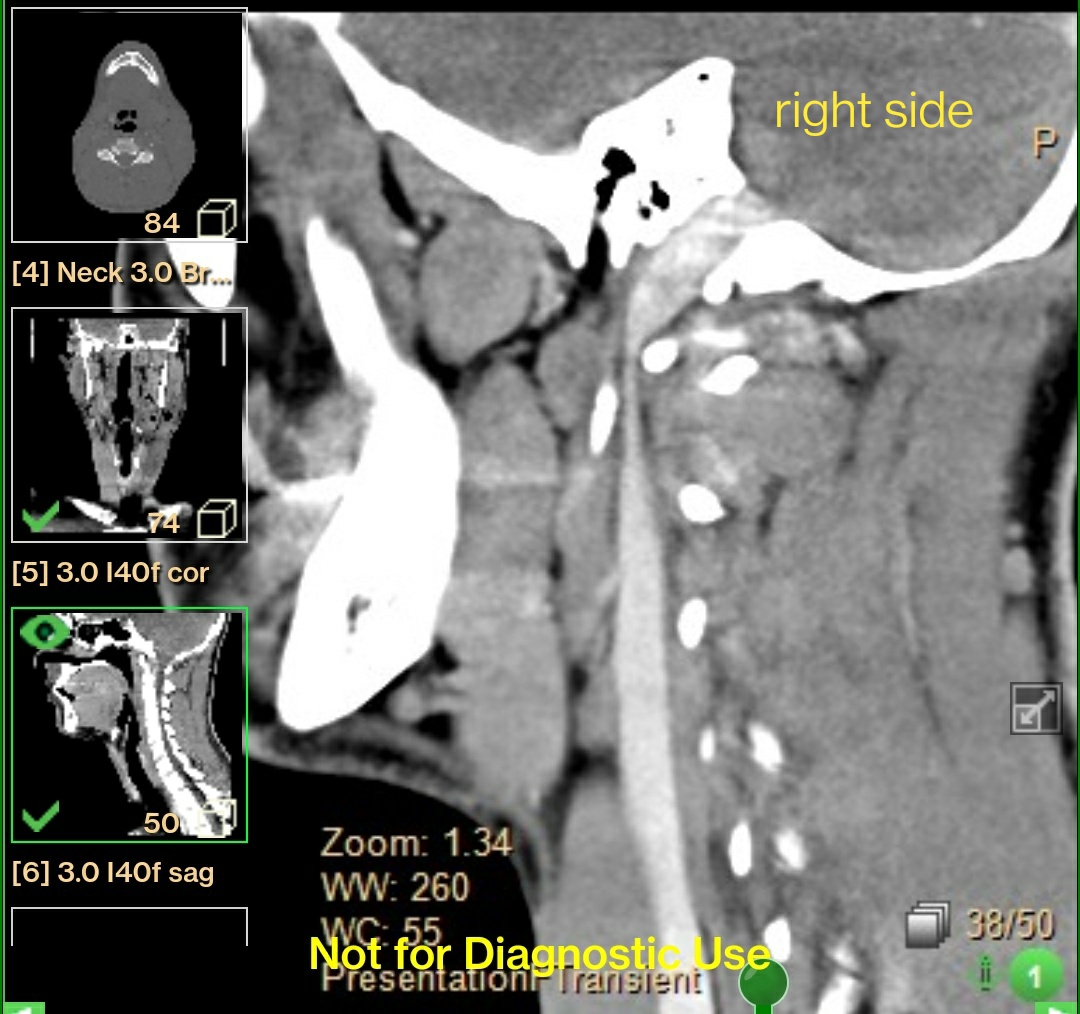
What I’m not sure about is what is causing the primary compression. Maybe someone else can chime in but from my very inexperienced eyes it looks like C1 is pushing your IJV and is causing the primary compression. This is not to say you don’t need the styloids removed, I believe you do, but you may also need the c1 shaved down a bit to remove that compression.
@11bravo , I agree with what @elijah says, there’s clearly compression with your C1 process & styloid process, whether removing the styloids is enough it’s impossible to say, but I certainly think it’s worth pursuing with an experienced ES doctor. Some doctors will review the images, like Dr Cognetti & Dr Samji, otherwise not sure which doctors you’ve reached out to on our list, but in FL Dr Jeffrey Scott Magnuson & Dr Rui Fernandes have done quite a few surgeries…you can search in the discussions for any doctors to see what discussions there’ve been about them if you’ve not already. It’s a shame that Dr Hepworth in Colorado isn’t taking new patients right now as he’s so good with the vascular ES…
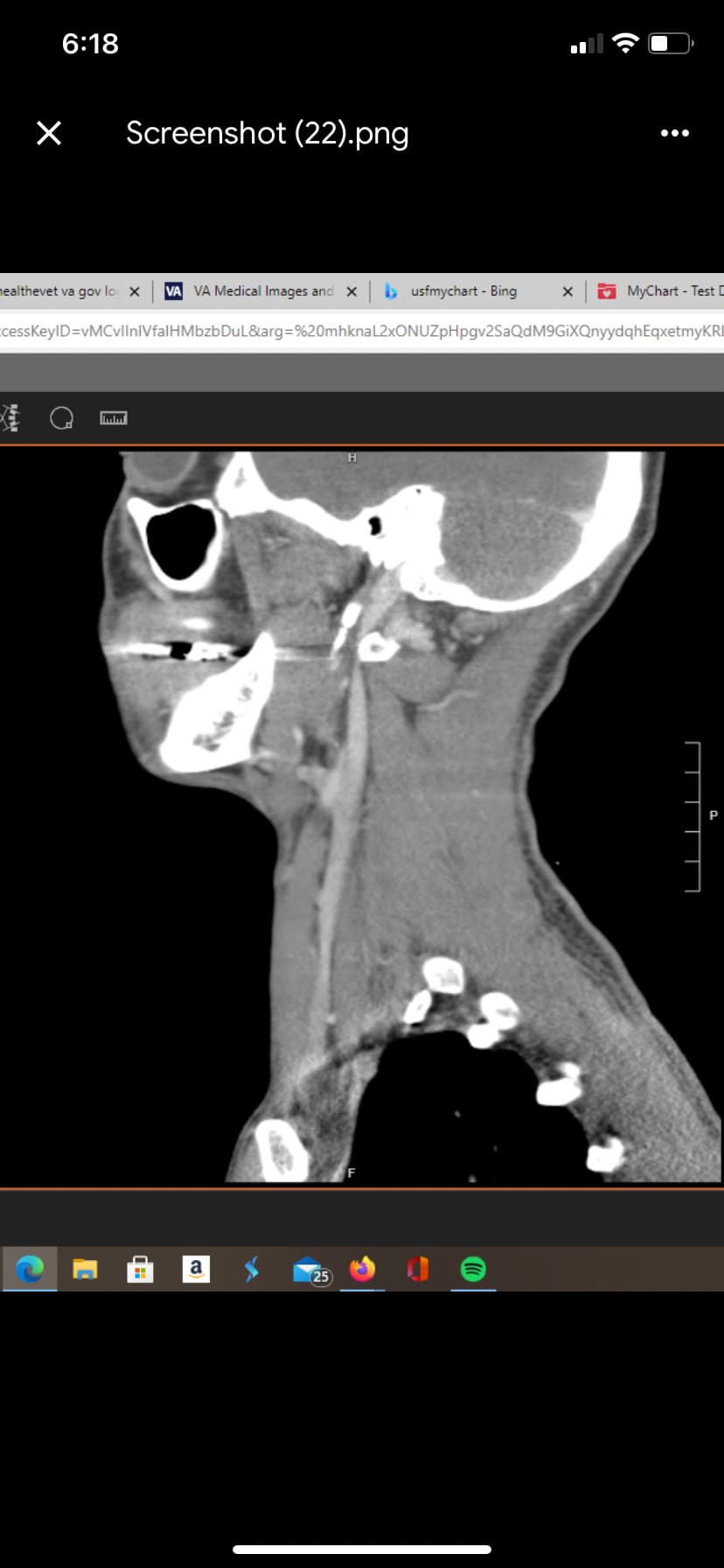
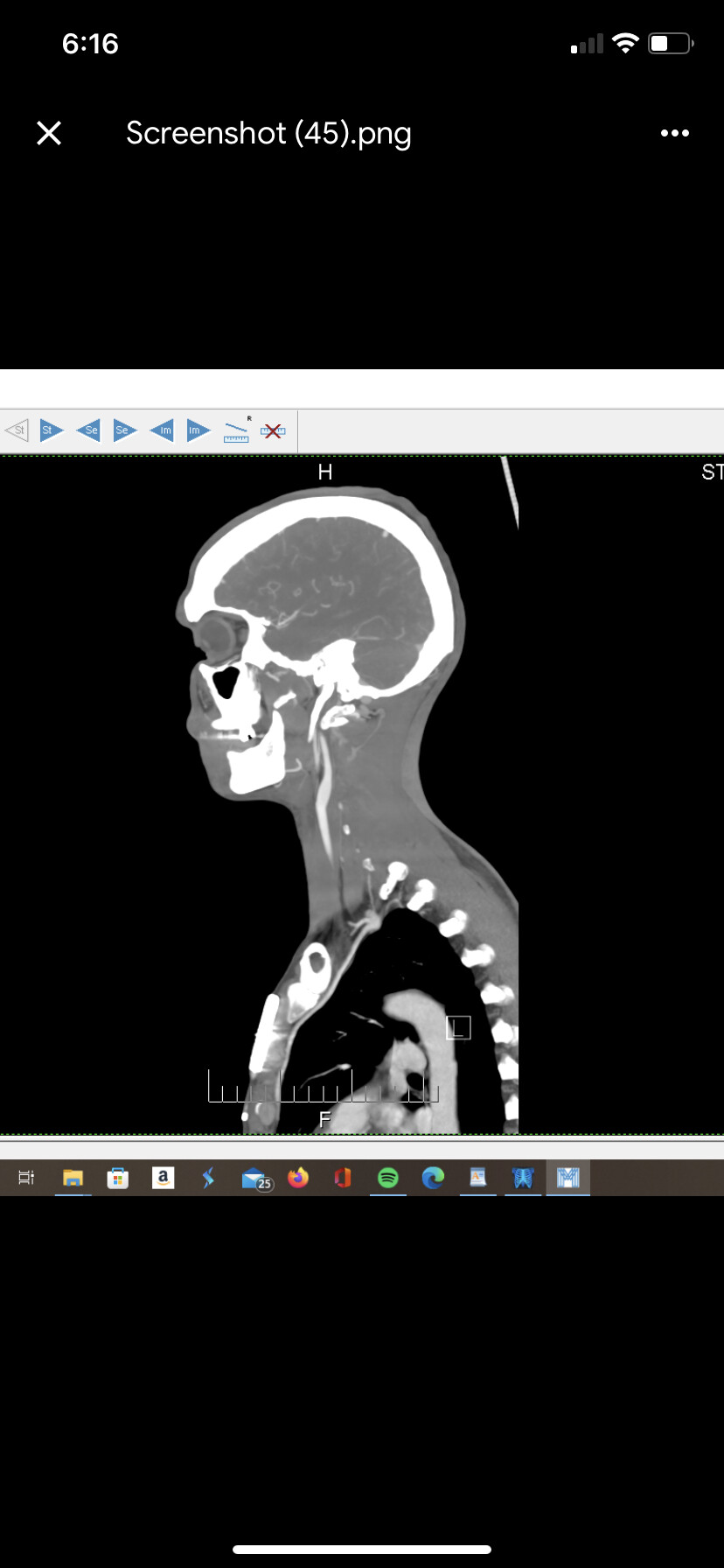
It’s funny you mention that. I’ve been saying for years that I think my c1 has translated forward. It definitely looks looks like to me that the ijv wraps around the c1 causing compression vs the styloids coming back into the vein. I’m sure the are an issue but I’m hopeful to figure out if I can fix the c1 will the styloid no longer be an issue. When I mentioned to my doctor about the c1 translating forward compressing the vein he said I’d be dead as the artery would be compressed first. Clearly any anatomy picture shows the vein closer. Your observation definitely seems like a good one for sure. Here’s a few more that seem pretty cut and dry that there’s an issue.
Thanks. I’ve got an upcoming appt with Dr Jonathan Morgan in Clearwater and hoping to hear back from Dr. Anthony Brunnell in Jacksonville. They’re both within a couple hours drive so I’m hoping they are a good start. I’d be happy if someone would just look at my dang images I bring to every appointment. Fingers crossed
Those are good images. I cannot tell you if c1 is definitely the primary compression, you’ll need testing for that. There are also many more members on this forum who are more familiar with scans and will have better insight than me. I will say, however, that it’s very rare to only have the c1 transverse process resected without a styloidectomy. Especially in your case where they are clearly calcified and elongated.
I think it’s a no brainer that your styloids need to go, the question is if you also need c1 work done as well.
I’m somewhat in a similar situation, however, I’m pretty set on just going for the styloids first and then seeing how I feel before deciding what to do next.
Ya I’m hopeful my appointment will give me more answers than questions. Was your original surgery pretty invasive? Are you able to palpate your styloids externally on the side of your neck? Did you have any headaches or continued headaches from the styloids. I ask because I had a bad neck injury and thought my migraines, dizziness, foggy head etc were associated with the injury but now I’m wondering if it’s the styloids. Unfortunately I’ve got an array of ailments that seem like the symptoms can overlap. Hopefully getting styloids removed will let me know for sure
My first surgery was through the neck. They removed most of my left styloid but didn’t go to the base of the skull.
My symptoms are really bad facial pressure, more intense in the front of my face. Dizziness, GI issues that only started after this did. Tinnitus. Burning skin on my face (it triggered my rosacea). Neck stiffness and pain. Double vision and blurriness.
I actually don’t have surgery pain. Was actually pretty painless and I only took one oxycodone while I’m the hospital. I have some residual minor numbness by my left ear and lower cheek and some first bite syndrome but honestly, it’s not bad enough that I even think about it.
Here more of my pictures from my post op CT scan.
You can see where they cut my left side but you’ll also notice that my styloid comes down a lot more straight than yours. They’re also in an insanely close proximity to my C1 lateral mass. Left side is essentially touching.
I’m glad you at least got some relief. Any idea why it elongated or was it something you were born with? When you’re miserable any relief feels like a huge leap forward. Where is your surgeon located? Did the surgeon think you needed the transverse process shaved down as well? Do you have any images on left post op that show the vein?
There are several theories as to the cause of styloid elongation:
Tonsillectomy - scar tissue builds up & puts pressure into the area of the neck where the styloids are so styloid(s) elongate/thicken to strengthen the area
Head/neck injury which causes the brain to think it needs to “shore up” the supporting tissues in the neck.
Hormone imbalance or parathyroid mishandling of calcium absorption
Hereditary component. We do have some members where one parent has ES & one or more of that parent’s children also have it.
Right now there’s only theories. I’m leaning towards whiplash I had a few years ago during skiing and I used to crack my neck a lot, but that might not explain why it started so suddenly. Going from feeling 100% fine at day and waking up with all my symptoms the next morning. So I’m honestly not sure what happened that triggered it so abruptly.
It’s more likely that there’s multiple factors at play here and some we will figure out with time and others we may never.
My first surgery was in March this year in NYC at NYU lagone. My surgeons were great and amazing people. The staff and hospital were amazing. They are just not experienced with the vascular ES condition so they didn’t take out all the styloid.
Initially they were going to shave my left C1 transverse process as well, but during the surgery they didn’t feel like it was causing the compression so they only did the styloid. If they took the styloid out at the very top it may have done the trick for my left side. My right side is my dominant side so we need to fully free that vein.
For now, I’m opting out of touching the C1 and hoping that a good double styloidectomy with Dr Hackman will do enough of the job.
I’m fully prepared to have to do more work after. Be it another balloon angioplasty to open the collapsed vein, c1 work and / or a stent. Only time will tell.
Ya the million dollar question is my life story lol. I’m glad you’ve got a network set up for you to get this squared away. Not knowing if this is the actual cause is the worst. Hopefully next month I’ll have more answers.
Yes that’s what he said to me also, he said he was going to remove the diagastric muscle on the left side, I love to be different from everyone else, he told me he’d done this particular surgery 20 times
I have experienced all of these! I have Jugular vein compression, and just got a styloidectomy and jugular de-compression about 2 moths ago. Unfortunately I’m experiencing some setbacks, but I’ve read such encouraging stories on this forum and know that hope it out there! Have you seen a neuro-opthomologist about the double vision? Curious too if you see full double, or if it looks like more of a halo around things. Mine is mostly halo, unless it’s text on a big screen, and then it looks like letters stacked on top of each other.