Yes, that’s exactly what I’m trying to do( I.e. Get on cancelation lists). Due to their specific scheduling requirements I am not on the cancellation list yet for Dr H as they may require me to fly to Colorado to be added to the surgery schedule( although there is a slight chance they may be changing this requirement to book in person soon). I have another consult with one of the NP’s in a few days to review new imaging so may get more info then. I’m not actually in a good position to do any traveling as I can barely leave the house. However, since It looks that I can’t get the surgery locally anyway, it seems it’s going to be necessary. Basically I can do it as a mess, running on adrenaline and then just crash myself for several days/ a week afterward as a result. I’ve done that before to get through other medical tourism trips, I’m just trying to do it as little as possible as I think it’s unhealthy. That being said, for surgery itself, it seems worth it. I don’t know if I’m going to find a viable alternative to Dr H but I would also consider moving temporarily if a surgeon would be able to get me in sooner, so either Colorado or elsewhere. I can’t remember if I asked, but can I ask which surgeon you went with?
@jyoti Thats interesting, I’m very curious which Drs said “head first”? Was that Dr B’s opinion? When I had my first consult with the NP at Dr Hep’s office, she said that bc these compressions can aggravate one another, that sometimes fixing one can lessen the severity( or even eliminate issues with) the other. She did lean toward “head first” but she also acknowledged that she’s seen things work in the opposite direction for some, and admitted that in general, it can be hard to predict which compressions are wreaking the most havoc in advance. She definitely did recommend doing one at a time though. I did speak to one ES patient who actually said she wished she had had the MT procedure first, although it wasn’t entirely clear to me why/ or I just didn’t thoroughly clarify that with her.
Do you have allot of unilateral leg pain? I have allot of pain sort of near the front hinge of my hip and down into my L leg( also lots of hypertonic pelvic floor type stuff) but I don’t have leg swelling or serious mobility issues. All I know is that my CTV result is abnormal and showed narrowing of left iliac, but I haven’t had the additional imaging to gauge the level of compression yet. I find it very interesting that I have the MT on the same side as my bad ES symptoms. That’s interesting what you said about patients not benefiting so much in the autonomic nervous system department from that procedure.
What level of compression was identified in the other imaging you had? I think if the compression is significant, it may be worth it.
Since getting confirmation of the MT( even if I don’t know exactly how bad it is yet), I have wondered if this issue might in-fact be a bigger problem than I previously appreciated but I don’t know. I sort of try to ignore my lower body symptoms, because my face and head symptoms are so much more, well, in my face if you know what I mean.
I haven’t consulted with the MIP’s center yet but I’m scheduled for a tele consult in 3 months and trying to get in sooner. I was thinking along the same line as you, in that, if the wait is long for styloidectomy, maybe I can get this other thing out of the way and get some relief. One big motivator for me was hearing that for some people MT can cause pretty significant fatigue which is currently my worst symptom. All that being said, I am mostly convinced that ES/what’s happening in my neck/ head is the main driver in my case and atm, I would rather get the ES surgery first if I could choose. Frankly, I don’t love the idea of having anything implanted in my body, even just a small piece of metal, but I do like that it’s maybe a less invasive surgery. Also, most people that I’ve randomly spoken to about it seem to not regret the procedure at all/ say it has allowed them to start exercising again/have less fatigue and things like that.
That is frustrating about Dr Nakaji. I mean, I’m of the mind that I don’t want to have surgery with anyone who doesn’t want to do surgery on me for whatever reason, but it seems that many patients in this population have some degree of MCAS as well as hyper mobility. Considering that I’m only in the midst of getting formally diagnosed with MCAS this many years in, it seems like something that often goes undiagnosed. Since you seem like an educated and self aware patient, you just happen to know about these things. Also I swear, not everyone seems to like the more educated patients (especially female ones). Not making any assumptions about Dr Nakaji but that’s a real thing I’ve observed.
I feel a-little silly frankly that I didn’t figure the mcas part out sooner, it’s just hard to know exactly what’s going on when you have so many symptoms and feel generally dreadful all the time.
Since going off my Quercetin and other allergy meds( my Dr said I could stay on cromolyn) for the last 4 days, I’m amazed by how much worse I feel. I couldn’t even sleep last night!! My restless legs are back, weirdly my palms and soles of my feet are itching(?), overall pain is up, and this is while I’m still on the cromolyn! I started noticing that old feeling of having anxiety and shakiness after eating yesterday and my whole nervous system seems to be freaking out. Thankfully, I can go back on my regular mcas stuff after the test tomorrow. I feel like I’m in hell right now, but trying to observe things like a scientist. It has erased any doubt about how much things like quercetin are actually doing. As bad as I am even on the stuff, it’s crazy to think I used to actually live like this. Sometimes we don’t realize what’s helping until it’s taken away.
Anyway, I know some severe MCAS patients and I can sort of understand a Dr not wanting to do surgery on someone who goes into anaphylaxis all the time/ can’t tolerate medications used during surgery, but I understand it less in your case. The chronic systemic type of inflammation and symptoms people like us experience are awful but it seems like our bodies are admirably working very hard to keep us out of the red zone.
Also, I could also never have surgery without doing a vibe check of a surgeon in advance. That seems crazy. Maybe you’re the same= bc I feel like the vibe check is the #1 most important thing.
Ha, it does feel like a rats nest! ![]() I have them living in the middle left side of my neck and in my left face/ head for sure.
I have them living in the middle left side of my neck and in my left face/ head for sure.
I’m new to this forum so not familiar with what any ES patients have said about Dr B here, but he seems like one of the best in the game to me. His understanding of everything CCJ and neck seems unparalleled. The wait to see him seems maybe the longest of all though, so if you got in, that’s great.
To be honest, I tried to submit to him for a case review to start but two of his office staff sent me weird “we know this isn’t what you wanted to hear” emails, letting me know they were not accepting me as a patient due to my out of state insurance coverage. It was weird bc I was prepared to pay out of pocket for the report and had recently changed my insurance to a PPO plan bc it offered more coverage. I did let them know that I wasn’t actively seeking a fusion right now, so they may have declined me for that reason. I tried to ask some additional questions and they just ghosted me, so I basically stopped trying. I’ve been more focused on Eagles specific surgeons since but it was weird. I’ve watched videos of Dr B talking about CCI stuff, and he low key seems like the man so I think you’re making a very smart choice/ makes sense incase of possible CCI emergency. Out of curiosity, why do people or ES patients struggle with him? I mean the office and scheduling seems to be a mess but that’s as far as I got.
Ugh.. thinking about CCI destabilization is a full on nightmare. I truly hope that doesn’t happen for either of us.
Can I ask why Osborne is “dreamy”? I had a consult with him and I do not understand.
I know this msg is long, but I’m also curious what your relationship with tethered cord or OTC is? I know my eagles and MT is confirmed but I am afraid that I might also have some degree of tethering. I keep going back and fourth about if everything I have could be caused by VES, MT, etc and I truly hope that’s the case but I keep wavering.
@Glitterbats - @jyoti didn’t promote Dr. O for patients in the situation you both find yourselves but noted that for the right patient group he “sounds dreamy”. I didn’t recommend Dr. O for you but only suggested him as a Dr. you could consult since he is extremely knowledgeable about ES & especially in unusual/complicated situations.
I know that Dr. H will fit cases he considers more urgent into his surgery schedule more quickly than those he feels can wait so it’s good you’ve got another consult w/ one of his NPs coming up soon.
@Isaiah_40_31 I’m kindof confused because I consider @jyoti and myself to both have unusual/complicated situations. It was not my understanding that he was the right surgeon to go to if you have complex VES and co-morbidities such as CCI happening, which is what I think would make an Eagles case complex or unusual but correct me if I’m wrong as I’m new to the ES world. When I consulted him, the depth of conversation that we had beyond my styloids being calcified was very limited and when I asked him for a script for imaging( beyond a basic neck CT) to help identify the vascular type of ES I pretty clearly have, he was not willing to write it( told his assistant to tell me to get it from “the other ES surgeons” I am consulting). Because I have such severe fatigue and have been so debilitated, it has taken me months to get another Dr to write the needed scripts and complete the imaging( my last test is tomorrow) which has slowed things down. I understand if this is something that needs to be discussed in direct messages, but I was genuinely asking why he is considered dreamy by some because was not understanding.
I’m sorry I tossed off the term ‘dreamy’ because it connotes too much. More simply put– I have heard a lot of people rave about how both kind and competent he is–if you have a fairly straightforward ES. Your experience sounds like one that confirms the straightforward part.
@TML It’s good you know about the ES being a big issue. I’m curious, if you had a digitial motion x-ray or upright MRI, both using a specific CCI protocol? I’m definitely not saying you have it of course, it’s just a bit of hassle to get the specialized imaging required( usually one of the two above or both) for a formal CCI diagnosis which is probably why allot of people suspect it or are self diagnosed.
I agree that allot of ES symptoms and CCI symptoms are the same though. One of the lame things about CCI, is that it seems to cause any symptom under the sun.
What you refer to as acute (pure) CCI is often called post traumatic CCI and sadly, the ligaments do not heal and tighten correctly on their own which is what leads to CCI from my understanding. Those tiny upper cervical ligaments do not have fantastic blood supply to begin with, which is why if they are in damaged in a significant way, it can cause real long term problems.
This is why some inject stem cells into these ligaments to try to try to get the body to heal them. Injecting facet joints and improving posterior stability can help compensate for the ligamental injury as well as a different approach. Or of course, fusion is an option too. Posterior cervical prolo was how I finally got my atlas to stop going out because other approaches didn’t help, however, I still identify with having CCI bc I have alar and transverse ligamental damage. Also I’m not asymptomatic ofcourse, but I think *maybe* that the styloids are now my primary problem.
I actually do have post traumatic CCI( have a head trauma history) but also seem on the hyper mobility spectrum. I think that can be true sometimes of the people with post traumatic CCI. Maybe we just don’t bounce back the same way from head or neck traumas compared to less bendy people. ![]()
Anyway, I’m not sure if I missed any questions(?) but agree that ES and CCI impact one another allot and I hope you will get great results from ES surgery.
@Glitterbats unfortunately in Canada we have very few DMX machines and only one upright MRI machine (which is the opposite coast from me). I’m very inflexible and my autoimmune panels (particularly RA) were negative, so I don’t have any susceptibilities to CCI. I was bedridden for 2-3 weeks due to dizziness before I popped the top of my neck so I think it’s just making things worse for me.
I have multiple things going on.
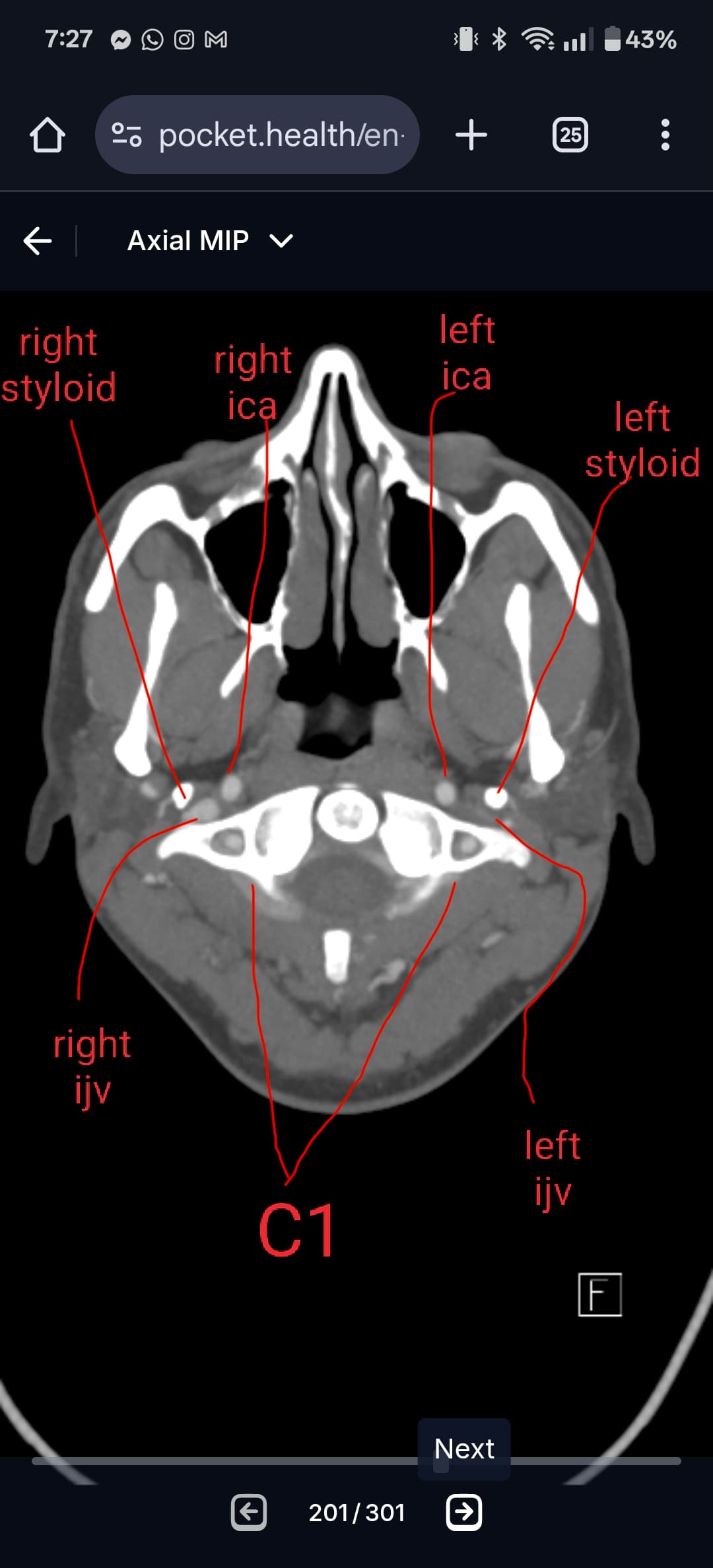
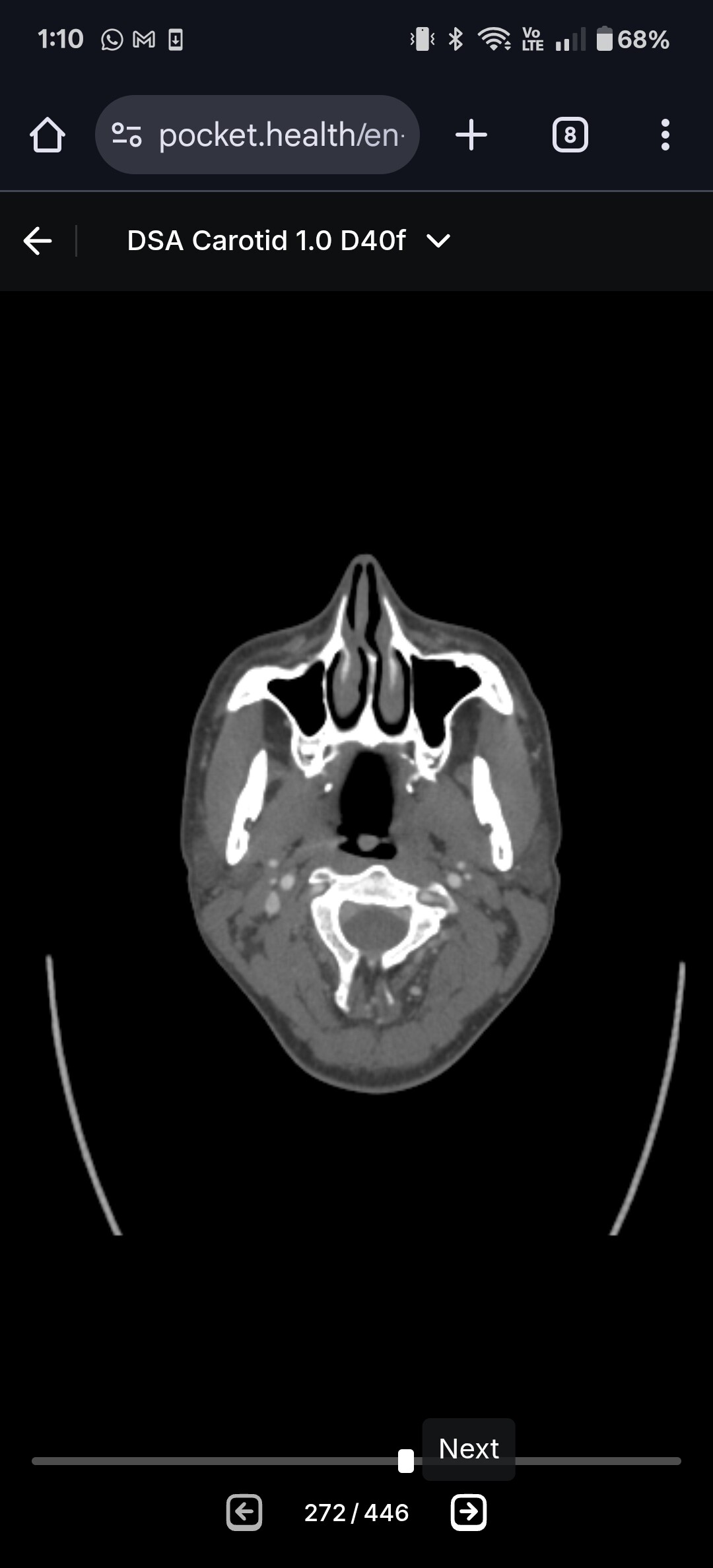
#1 both IJVs compressed between styloids and C1 (especially left side). Tip of left styloid is 1mm from left ICA. Both styloids are 3.3cm in length.
#2 both IJVs compressed between SCMs and anterior scalenes

#3 left greater horn of hyoid digging into carotid sinus area, which has landed me in the hospital multiple times due to stroke-like symptoms.

#4 right greater horn striking and sometimes getting stuck on my vertebrae

I’ve been diagnosed with both eagle syndrome and hyoid bone syndrome. Haven’t diagnosed with scm syndrome or scalene syndrome, but I think it’s possible. And each come with their own symptoms. The IJV compression is causing me intracranial pressure symptoms and also persistent oscillating vertigo which is awful. Haven’t left the house in a long time because every time I stop a motion event (car ride, elevator, treadmill, etc) I feel like I’m still in the motion for days. IJV compression is known to cause persistent oscillating vertigo.
The hyoid bone syndrome is causing my stroke-like symptoms. Simply moving my tongue around in my mouth (which moves the hyoid) makes me dizzy and causes my body to tense up.
So although I think CCI is possible in my case, I have so much crap happening in my neck that I know are directly causing my symptoms (i.e., laying down in bed without head movement while simply moving tongue in mouth triggers dizziness). I think if I have any CCI it’s are a consequence to the trainwreck I have going on (especially since I didn’t self-injure my neck until a couple weeks after symptom onset).
Hoping my left styloidectomy and left greater horn resection fixes me up. If not then we are going to do a right styloidectomy and right greater horn resection.
I think once my styloids are out the SCM/scalene problem will get better. I’m a fairly unique ES case where I actually haven’t lost any of my neck curve (which would also reduce the likelihood of CCI). And actually, although it wasn’t identified as such, I think my neck curve might be too much (i.e., hyperlordosis):

I’ve spent many years slouched at a computer (shoulders dropped with cervical extension; “hinged” neck). This would be the best postural position to open up the styloid-C1 space. So I suspect I subconsciously engaged in the posture because proper upright posture with head tilted slightly down to look at my computer (I’m a doctoral student) would cut off the jugulars at C1. So I think my styloids have caused horrible posture for my whole decade of university studies.
The major problem with chronic cervical extension (particularly in combination with forward head posture) is that it puts strain on the SCMs and anterior scalenes. These muscles become predominantly stabilizing muscles when they shouldnt be. My deep anterior neck flexors are mega weak - I can’t do a chin tuck without the SCMs taking over, little lone do that exercise where you lay on your back and slightly lift your head off the ground. The only exercise I can do where I feel some engagement of deep neck flexors is isometric flexion exercises, but even then the SCMs usually take over. And I can’t properly hold chin tucks or good posture because my intracranial pressure symptoms get horrible (due to cutting off IJVs at C1). So I’m really hoping that with styloidectomy(ies) and some following physio that I’ll be good to go.
This is the treatment plan that I think makes the most sense to me:
Left styloidectomy+ left greater horn resection → physio → if physio doesn’t work than right styloidectomy + right greater horn resection → physio → if physio doesn’t work than look into neurotoxin for SCM/scalenes → if nothing works than look further into CCI
My ENT calls my left styloid and left greater horn the “low hanging fruit” so hopefully I’ll improve significantly with them out of my neck
@Glitterbats I’ve sent you a pm about Dr B.
@tml Yeah, I live on the west coast on the US and had to fly to the east coast for CCI diagnosis, so I can empathize. But to be fair, the only medical progress I’ve really made had been the result medical tourism.
I feel like allot of the information you have about CCI is confused and/or there are many incorrect assumptions being made.
I was not positive for anything on any autoimmune panels/ have been tested( don’t have RA) and many people with CCI don’t. Those tests are also extremely flawed and many people with connective tissue issues and autoimmunity do not get formally diagnosed with a test. Even classic EDS is considered to be a diagnosis of exclusion since there is no genetic test for it.
There is also not a direct correlation between loss of lordosis and CCI even if they can overlap( such as in cases of whip lash or head/neck trauma). There are a subset of people with CCI who have an exaggerated lordotic curve. Some have a normal curve. Hyperlordosis can be the bodies response to chronic forward head posture( If they have CCI, this would be if their bodies strategy for stability is extension rather than flexion).
I think you may have mentioned something about not being super flexible somewhere also, if so, I would search for the term “tight zebras” in any groups for people with hyper mobility/EDS. For some people, the body becomes very tight rather than looser as a direct result of hyper mobility.
Anyway, I’m not saying you have any of these things! Just don’t agree with the reasoning for why you don’t.
If you can somehow find a CCI literate upper cervical chiropractor in Canada( I’m sure there are some) who are familiar with complex cases/people who have other conditions like ES, it might be worth while having some imaging to see if your atlas is “out”. Normal people without CCI can still have their atlas “out” and it can cause allot of problems. It doesn’t involve any cracking and is a vey tiny adjustment of C1 only that can make a big difference for some/ This type of Chiro does not adjust any part of the body accept C1 usually.
Anyway since the Eagles is confirmed, I hope the styloid removal will help allot.
Thanks for that info @Glitterbats .
Would the chiro be a NUCCA chiropractor?
Also, how are “tight zebras” diagnosed. Genetic testing?
So some people do Nucca or Blair. I prefer Atlas Orthogonal( AO) because it’s done with a machine rather than a human. There is also “Advanced AO” which I’ve never done. There also some other type of upper cervical chiro but those are the main ones.
To my knowledge there is no genetic testing for hEDS/ EDS but some specific subtypes like vascular EDS and some other connective tissue diseases can show up on genetic testing but most of those are pretty rare.
Zebra is just anyone with complex health issues so doesn’t automatically mean hypermobile although many seem to be. Something like hEDS would be diagnosed based on meeting specific criteria and formal evaluation in addition to excluding other diagnoses. You could also learn more about tight zebras in particular maybe in some EDS support groups or something.
I think there’s a NUCCA in my area so I’ll have to see if I can get in with them. My vertebrae aren’t straight (particularly C2) so perhaps they can do something with it! I was told by neuroradiology that it’s normal to see some off-centering of the cervical vertebrae, but perhaps there’s more to look into there.

That could definitely be could be worth checking out. I would just research that chiro extensively/ check their reviews and ask if they have post grad training in CCI and/or are knowledgable about complex cases. You could still have luck with a very good one that is more normal but they are not all created equal. I don’t think mis-aligned upper cervical vertebra are a small deal at all and was wondering today how many people end up having their already misaligned C1 shaved when getting something like styloid surgery but I’m not a Dr.