I played around with 3d slicer and found that it could do some of the images easily and others labeled as ending in “topogram” with great difficulty. I assume the non contrast images were labeled correctly as sagital, coronal, and ap and were easy for 3d slicer to handle, because when I added topogram to 3dslicer, it slowed down considerably. Either way, I got decent images totalling 385 altogether. This is both non-contrast and contrast images together. Not sure what differentiates them in the file labels? I uploaded decent images that were non-contrast coronal and all non-contrast views, I believe. My styloids were long bilaterally. I cannot tell if styloids are impinging on vessels. One ENT doctor did not seem to think so, but again his training in this area is somewhat limited. He basically just knows how to remove the styloids safely from inside the mouth when he can palpate them with his hand.
I have been having cranial nerve problems for a long time it seems. I have had many peripheral nerve surgeries including TOS release bilaterally, suprascapular nerve release bilaterally, dorsal scapular nerve release bilaterally, auriculartemporal nerve release bilaterally (by ear), and many others outside the head and neck. I think I have vagus nerve dysfunction in addition to POTS, making it difficult to concentrate on things and possibly making my fight or flight response go haywire increasing muscle tension everywhere, hence all the peripheral nerve surgeries to cut tissue away from nerves. I don’t expect doctors to diagnose anything besides the styloids unless I send out my CD images to UCLA, Stanford, and doctors mentioned on this forum. It is tough to know if I should just cut the styloids out and go from there to see what symptoms remain or try to travel and get all these tests before cutting out styloids to get the exact right operation which could take awhile. In addition, I have other nerve surgeries to add to the mix that are a little less important than dealing with ES, but still important.
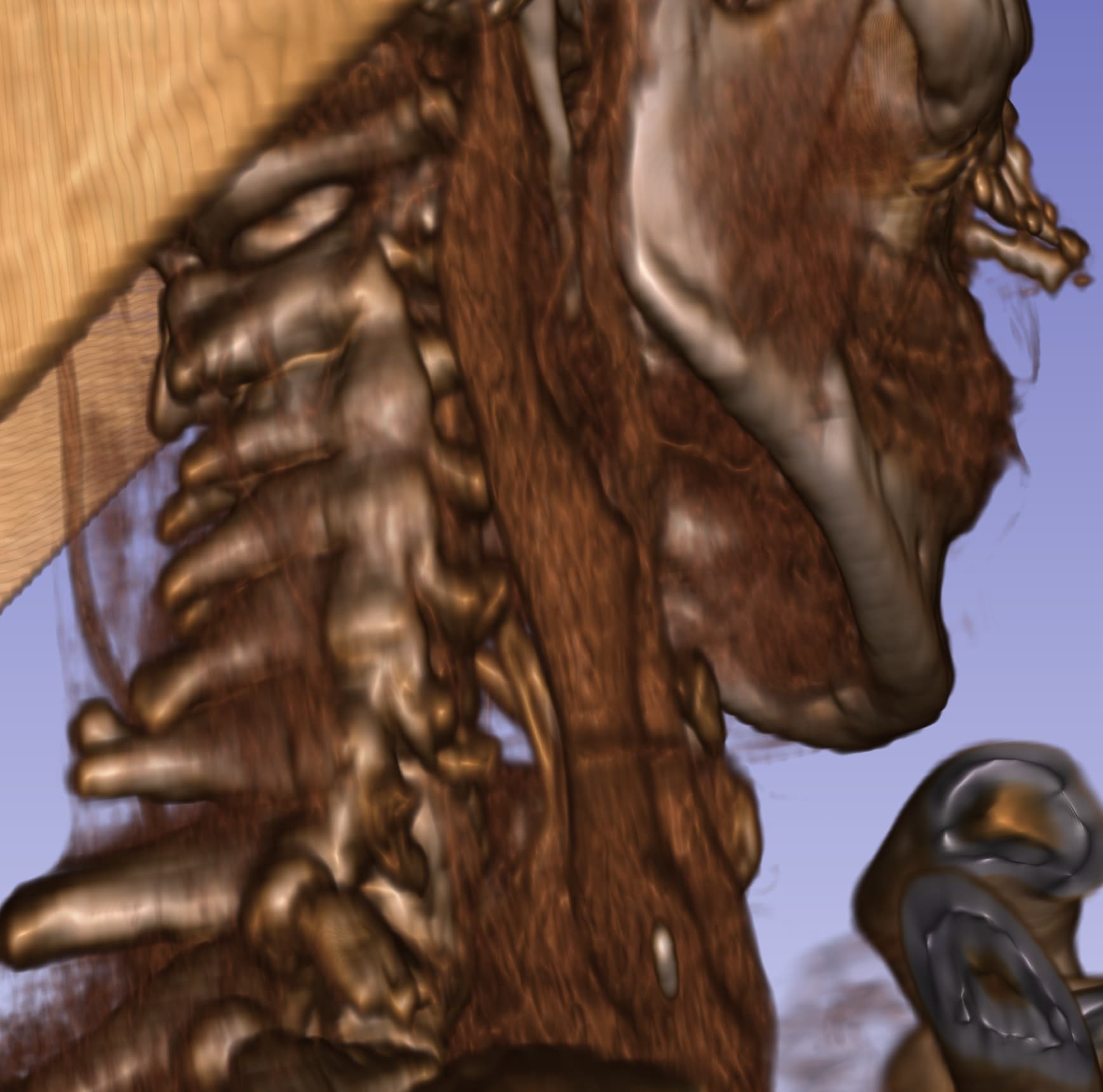
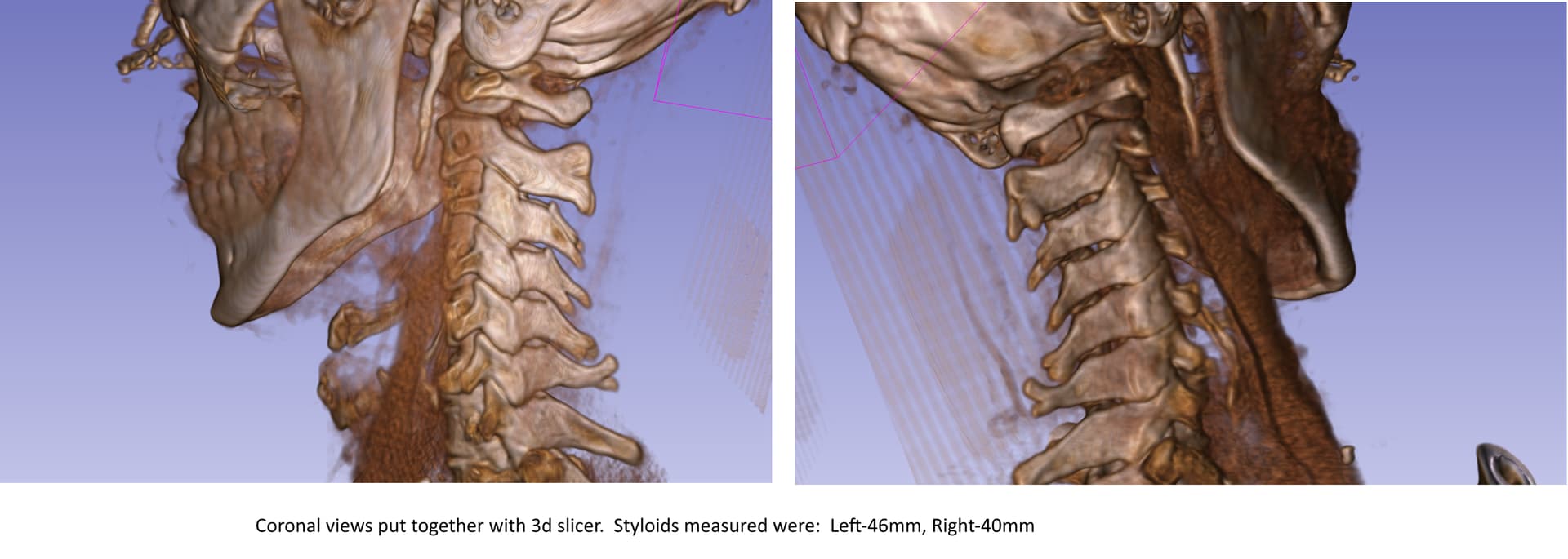
Wow, they look pretty long styloids! The gap between the styloids & C1 looks a reasonable size which is where there’s often compression, but on the second image you’ve posted it looks like there could possibly be some compression of the IJV higher up near the top of the styloid & the skull base- I’m sorry I can’t label the image for you, & it’s not that clear so I could be wrong!
It’s difficult sometimes to know who to see for surgery & what tests to go for, but given you believe you have cranial nerve issues & that several of these nerves exit the skull right beside the styloid (along with possible compression of the IJV at the skull base), I’d certainly opt for external surgery and not intra-oral, with an experienced surgeon who can remove the styloid as close to skull base as possible. So worth consulting one of the experienced doctors on our list if you’re able…
Yeah, I thought so. I have the images uploaded to dicomlibrary, but I also downloaded the images in png format as well. Let me know if I should zip any files and attach to this post for more clarity. I sent the images to Nakaji to look at them. Hopefully, he can see any nerves and/or vessels being compressed near skull base.
Nice job w/ your 3D images, @jobby99! I agree w/ what @Jules said about your right IJV looking compressed up at the top. Your styloids look like daggers in your neck so no wonder your cranial nerves are irritated! I’d guess they’re longer than measured. I also noted that your left styloid is very thick at the top. There isn’t a similar image for the right one, but if it looks the same, it’s possible it’s causing IJV compression up by the skull base as Jules noted.
You can see on the right in this image how the IJV is flattened a bit. That can be indicative of some compression occurring. The left side is also a little flat/not round which could also indicate you have some compression on that side. Remember I’m not a doctor so this isn’t a diagnosis. It looks like your right IJV may be your dominant IJV. Not everyone has a dominant & non-dominant IJV but quite a number of our members seem to.
In this picture, it looks like the tip of your right styloid may be touching your internal & possibly external carotid arteries. That can also cause pain & sometimes stroke-like symptoms.
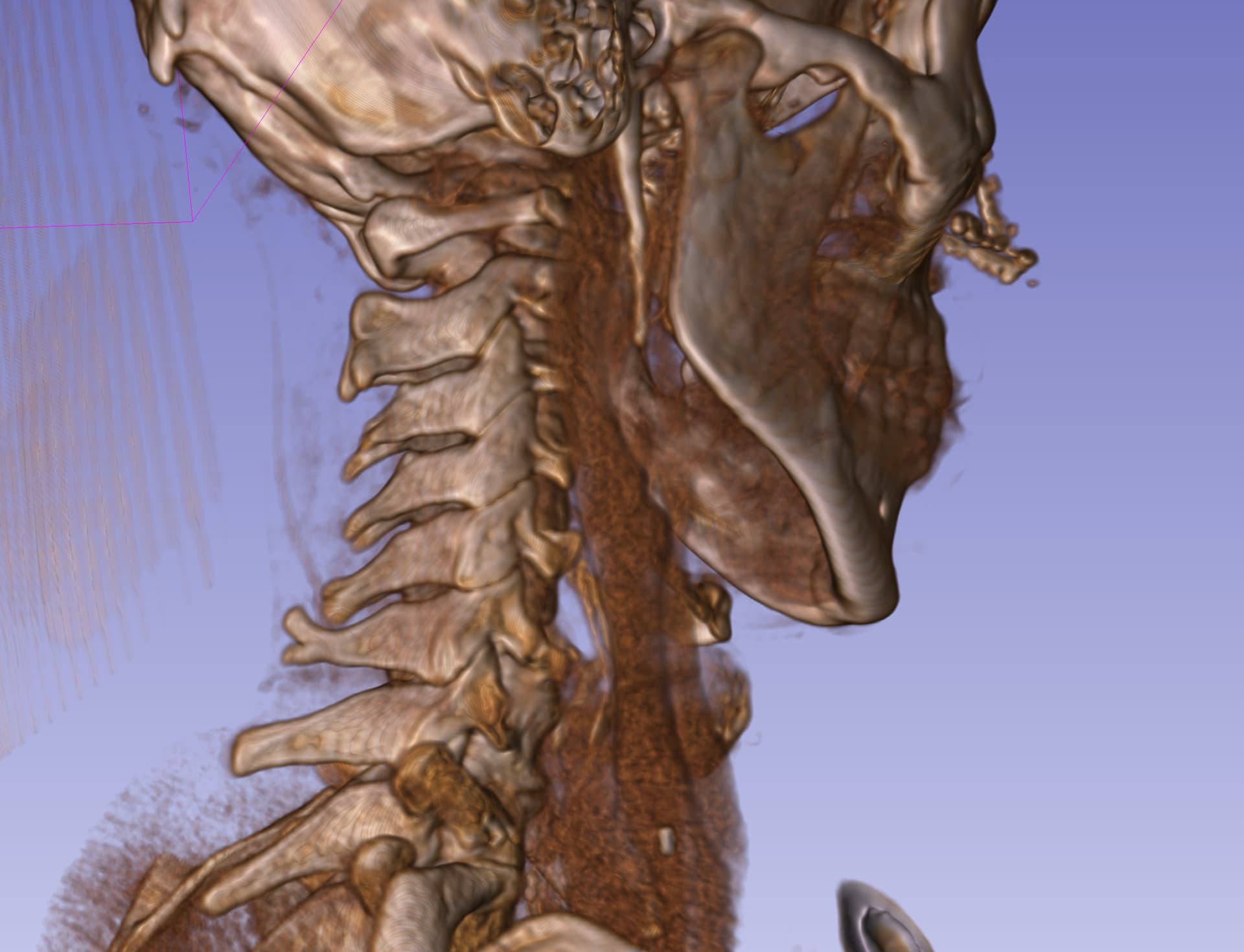
I also noted you’ve lost the lordotic curve in your cervical spine which is also the case for many of our members. That can push the styloids more forward & into the very vascular & nervy interior of the neck which puts nerves & vascular tissues at greater risk for irritation/injury.
Thank you for commenting. I am having trouble getting a CT Venogram that Dr. Nakaji wants, but can’t order probably because he can’t see me right away or do virtual at least. He must think that it is needed based on the CT scans. I totally agree with compression of the vasculature. It does look like the thicker bone is a problem. Hoping to see a more experienced provider soon to at least get more imaging and opinions.
Dr. Cognetti thinks I have plenty of room for IJV, so I guess I am good there. However, I do feel like not enough blood is getting to my head still. Here is another 3d slicer image of my styloids using their software to measure them.
I don’t think I am going to do anymore testing. Left was removed Oct 25 and Right was removed Feb 26. Both of my styloids have been removed to the point of normal length (about 1 cm), so I am going to wait and see if anything changes. I feel like right side is worse when it comes to jaw clicking, ear pain, and lightheadedness attacks happen when right side of neck feels odd. Overall, swallowing, throat and ear pain have improved. Still have eye blurriness when looking up, tinnitus, some jaw pain, headaches, and lightheadedness. Due to excessive wind in my area, I couldn’t do my follow-up appointment but I am sure he is just going to say it looks good. I had no swelling and incision is healing fine. I think I have a new hair coming out of my incision on left side, which is odd so I am already shaving over the scar 6 months out. The body does weird things.
I’m sorry that you still have some symptoms, but it’s not that long since your second surgery so there’s still time for more improvements…probably a good idea not to rush into any more testing, but see what resolves, it can take months for everything to heal as you probably know from your first surgery…
@jobby99 - I agree w/ @Jules about recovery taking a lot of time. It was a good 6 months post op before a lot of my symptoms were gone. I felt pretty good at 2 months after my first surgery, but definitely still had symptoms flares if I pushed myself too hard. By 4 months post op things were considerably better & after 6 months, I began noticing what remained disappearing gradually over the next 6 months. I hope your nerves recover more speedily than mine did, but it is a slow process.
At 1 month post op, you can still have internal swelling that’s putting pressure on nerves & causing symptoms. It’s usually 6-8 weeks post op before all the inflammation subsides. You can continue to ice your neck or maybe try heat now. Please continue to keep us posted as to how your recovery is progressing.
I think that most of my symptoms have been the same for the last few weeks. I notice that the right side is still more sensitive by incision. I have no swelling on my second styloidectomy on right side (never had swelling since I took a prednisone day before surgery). I still have the clicking in my jaw, but it doesn’t seem like it is a big deal. My carotid area on right side is still sensitive to any pressure (feel like I am being choaked), so that may still be improving slowly with time. Or maybe the hyoid bone attachments are just irritated.
I had another CT and my styloids measure about 2 cm. The surgeon’s report says 1 cm, so his estimation was just that. The styloids don’t appear to be sharp or interfering with nearby vessels at least in neutral position. Trying to see if I can get good 3dslicer image of C1 transverse process, but none of the views are very good. 3dslicer is hanging on my computer with some of the data sets dragged and dropped. It must be corrupt or data it can’t read. It was a CT Angiogram and all my vessels looked great on it. I wanted a CT Venogram, doctor wouldn’t order it. MicroDicom is a great free dicom viewer that can anonymize data and batch convert data. It is so easy to use. You just feed it one folder at a time to view dicom images.
Thank you for the information about MicroDicom (https://www.microdicom.com). We’ll start offering that as another means of procuring 3D CT images for our members who want to do that.
Have you done any investigation as to whether or not you might have CCI or Ehlers Danlos Syndrome (EDS)? The fact you’ve had surgery for TOS & several nerve release surgeries makes me suspicious that you may have one or both of those which could be causing some of the symptoms that remain.
People w/ EDS alone often experience compressions of various types lower down in the body i.e. May Thurner Syndrome, Median Arcuate Ligament Syndrome, &/or Nutcracker Syndrome. Even though MTS & NS are much lower in the body, the way they affect the blood flow can continue to cause the type of symptoms you have remaining.
Another thing you could look at is Superior Semicircular Canal Dehiscence Syndrome which can be caused by high pressure in the brain from IJV compression. Though all your remaining symptoms don’t fully point to that, some of what you’re experiencing does.
I have a lot of firewalls or difficulty qualifying to see any of the decision makers for CCI or Ehlers Danlos or IJV/IH/Vascular ES. I am thinking about just seeing someone from the listed doctors again who will order the testing, which Nakaji will not do. I am scheduled to get cervical MRI, flexion/extension x-ray, and meet with doctor who trained at Barrow Institute at Cleveland Clinic, so might shed some light on things. I know genetically I don’t have Ehlers Danlos and no relatives have it. I had a cousin with Chiari Malformation, but I had that checked ten years ago. I probably need to cut out all triggers for vestibular migraine or even migraine in general to make sure it is not some chemical cause contributing as well. I still don’t know why my left ear pops, but read the nerve can trigger opening and closing of the eustachian tube. Had 50,000 dollars of vestibular testing at Cleveland Clinic in 2010, but could have just been asymptomatic at that time. I was way more active and working long hours on my feet, so very different circumstances from the more lethargic sedentary me of today (due to nerve pain in feet). And no, I don’t have diabetes
It’s good news you don’t have hEDS or any of the other possible compressions I mentioned. The cervical MRI & x-ray that you have coming up will hopefully determine if you have any level of CCI.
I think your suggestion of cutting out all known possible migraine triggers is a good one. We had a member a year or more ago who had some major surgeries that didn’t help her symptoms resolve then she discovered that she’d had a genetic test done a couple of years prior to her surgeries that showed her body couldn’t process several significant medications. It turned out she was taking one of those & once weaned off of it, she got her life back. That’s to say that part of leaving no stone unturned when looking at possible migraine triggers should include any medications you take on a regular basis, too.
I’m sorry about your foot pain. Do you have neuromas or some other problem? Is the triple neurectomy to try to give you relief from your foot pain? Very frustrating to finally be retired but not able to be active!!
I think the foot pain is from having excessive fluid that tends to stick in my lower half. Unfortunately, compression stockings just irritate all the nerves just under the skin, so I don’t wear those anymore. Diabetic socks help a lot. Wish I had a simple solution, but nerve releases seem to be the best strategy so far. The triple neurectomy is typically done for hernias, because the mesh tends to get caught in the nerves in the area. However, only a few specialized surgeons have training to attach cut nerve endings to muscle tissue to prevent neuromas from forming in the future, which will lessen pain long term. Other surgeons may just try to “bury” nerve endings in muscle tissue, which is better than nothing but can cause pain long term.