@TexasEagleSuffer do you have access to your CT imaging? I just wanted to check out your hyoid for you. I have hyperacusis and I’m getting my left styloid but also left greater horn of my hyoid removed soon. So I wonder if your hyoid is causing any symptoms, especially where opening and closing your jaw (which changes the positioning of the greater horns) changes you tinnitus and hyperacusis.
1 Like
I do have them on a CD. Would need to figure out how to get the image posted here as I pretty much just use my iPad for everything now. ![]()
3 Likes
I think you’d need to purchase an external CD/DVD drive. Something like this:

I’m not sure if they make any that are compatible with iPads or not. And even if they do, I wonder if iPads are capable or not of opening the CT files (DICOM) or not on the CD. If you have an old computer or laptop around that has a CD/DVD reader built into it then that would be perfect, if not buying an external CD/DVD drive for a computer/laptop you have might be the best option. I think using a computer/laptop rather than the ipad would be better too because you could download Radientviewer and construct 3D models of your imaging once your computer has access to the CD
1 Like
I’m not sure what I’m doing wrong, but I cannot get anything to actually come up. when I I click on anything where there are images - A4, A5, A6, A7 A8, A9, I just get an error.


If you click on the A12 dataset, and then move your cursor to the right side of the screen, will it start flipping through the images if you scroll is your scroll wheel on your mouse? (Or double finger scroll if using a laptop)? Usually that lets you go through the full imaging
1 Like
@TexasEagleSuffer - How is your recovery going? You’re approaching 10 days post op. Any positive changes yet? It can take several weeks before those show up & a number of months for nerves & vascular tissues to settle down, but often there are some early initial improvements.
I’m sorry you’re having trouble getting your scans to post. I wish I could help but I’m terrible w/ tech stuff so have to rely on members like @TML & @Rosie who have more recently stepped up to help our members in that way.
1 Like
I wish that I could report more positive changes, but my Pulsatile tinnitus and my hyperacusis are worse than ever. Those were the issues I were hoping where I would see relief. The one area where I’ve seen positive change is with my neck pain by c1/c2. I used to get relief by turning my head to the right, opening my mouth wide, moving my jaw inward or pressing down on the top of my head. I only seem to get relief now by pressing down on the top of my head. I might get a little relief from moving my jaw inward.
One positive I can note is that I haven’t really had any pain from the surgery.
2 Likes
Hi I did a bit of research and it mentions that if you are reading direct from CD drive it maybe to slow to view multiple images and suggests saving to your computer and viewing them that way. I have no idea if that would work as unfortunately I’m not great with IT either. Hopefully what @TML suggested has worked.
2 Likes
Thank you. I just realized you repeated what you’d written above but you are still in very early recovery. It can take a couple of months for the post op swelling to go away significantly & as long as there is still swelling, there can still be symptoms because the inflammation continues to compress nerves & vascular tissues. It’s one way the body gets us to lay low for a while after surgery so it can put its energy into healing vs the activities of daily living plus any extra curriculars we decide to try. Hopefully in another few weeks you’ll start to have some positive changes. I am sorry that you’re still very uncomfortable. Did Dr. Welch shave anything off your C1 vertebra?
2 Likes
Below are the clinical notes from the surgery from Dr. Welch:
PREOPERATIVE DIAGNOSIS: Pulsatile tenderness secondary to styloid compression (Eagle syndrome).
POSTOPERATIVE DIAGNOSIS: Pulsatile tenderness secondary to styloid compression (Eagle syndrome).
PROCEDURE: Left cervical exposure for styloidectomy and drilling of lateral mass of C1.
SURGEON: Babu G. Welch, MD
ASSISTING RESIDENTS: Richard Shaw, MD and Darsh Shah, MD.
ANESTHESIA: General.
INDICATIONS: Mr. is a 62-year-old male with longstanding left-sided pulsatile tenderness that is lifestyle disabling. After consultation with my partner, Dr. Lee Pride, he was sent to me when styloid compression of the left jugular vein was very clear on noninvasive imaging. Symptoms are improved with cervical rotation, which is likely to move the jugular vein away from the styloid process and, therefore, we discussed with him the styloidectomy for treatment of his tenderness. He presents for that procedure today.
DESCRIPTION OF PROCEDURE: After obtaining appropriate informed consent from the patient with his wife and pastor present, he was brought to the operating theater and placed on the table in supine position. General endotracheal anesthesia was established along with invasive hemodynamic monitoring. The patient was placed in a horseshoe headrest, and his head was rotated to the right side with 2 blankets placed under his shoulders to allow for some extension. Palpation of the mastoid bone allowed for localization of a skin fold incision that would get us to the level of the styloid but a compression occurred. Once the incision was marked and the area was sterilely prepped and draped, the procedure began.
A #15 scalpel blade was used to make the skin fold incision. This was further developed using unipolar cautery on low energy. Blunt dissection allowed for visualization of the C1 process and just anterior and lateral to that was the styloid process. Between these 2 was the compressed jugular vein. Using blunt and sharp dissection along both the C1 lateral tubercle and the styloid process, all fascia and attachments were removed. The styloid was liberated approximately 1.2 cm, and this was then amputated using a Lempert rongeur. There was no bleeding, and then I focused my attention on the C1 process that was compressing the back portion of the jugular vein. Using a #1 Penfield dissector, I visualized the lateral process and using a 3 mm fine diamond burr on a high speed drill, the C1 process was drilled from behind the jugular vein, and straight curette and Lempert rongeur were used to complete the drilling of that process. Once this was completed, the decompression of the left jugular vein was identified. Any bleeding was stopped using bipolar cautery and we began closure. The wound was closed using 3-0 Vicryl sutures in the dermal layer and a running 4-0 Monocryl in the skin. The wound was dressed and the patient was awakened, moving all extremities with a decrease in his tenderness.
ESTIMATED BLOOD LOSS: 10 mL.
There was no specimen.
1 Like
Sounds like Dr. Welch did a stellar decompression surgery for you @TexasEagleSuffer! I’m very happy to know we may have another vascular ES surgeon for our list & especially one in TX where the pickin’s have been a little slim for our members there.
Please continue to keep us updated as to how your recovery is going. It will take some months which we’ve mentioned, but you should recover well. ![]()
1 Like
@TML I finally realized that I needed to download DICOM viewer in order to see the images - so I’m using a trial version. Please let me know if the images below help.
I am three weeks post surgery and I still have the pulsatile tinnitus and hyperacusis. My jaw has been more sore the last few days - particularly when I chew, but otherwise, I’m doing well physically. Dr. Welch is going to do another CT on Monday and then I will see him again on 07 Oct.



@TexasEagleSuffer - You’re still in very early recovery especially after having IJV decompression & a styloidectomy. It may take a number of months for you to begin feeling back to your old self. Two months post op was a definite turning point for me as my energy returned then, however, it’s also the point at which the symptoms from my remaining styloid began ramping up. Sigh…
Give your body some more time for recovery. Symptoms will come & go over the next months which can be frustrating especially when they’ve been gone for a while then return, but they will go away again. Nerves heal very slowly (up to a year or more in some cases) & your brain is still getting used to a new level of blood flow. It’s all a process that requires patience.
I’m glad you’re noticing some positive changes since surgery as that bodes well that your body is working at healing.
2 Likes
@isaiah-40_31. Appreciate the response. Is it normal for the Pulsatile tinnitus and hyperacusis to actually get worse before it gets better? It’s weird that last Sunday I thought I had turned a corner as I had a much better day, but Monday was worse and the last few days have been even worse. It is very frustrating.
@TexasEagleSuffer I can’t quite see the greater horns in these images.
Find the main body of the hyoid first and then travel up and follow the horns to their tips.
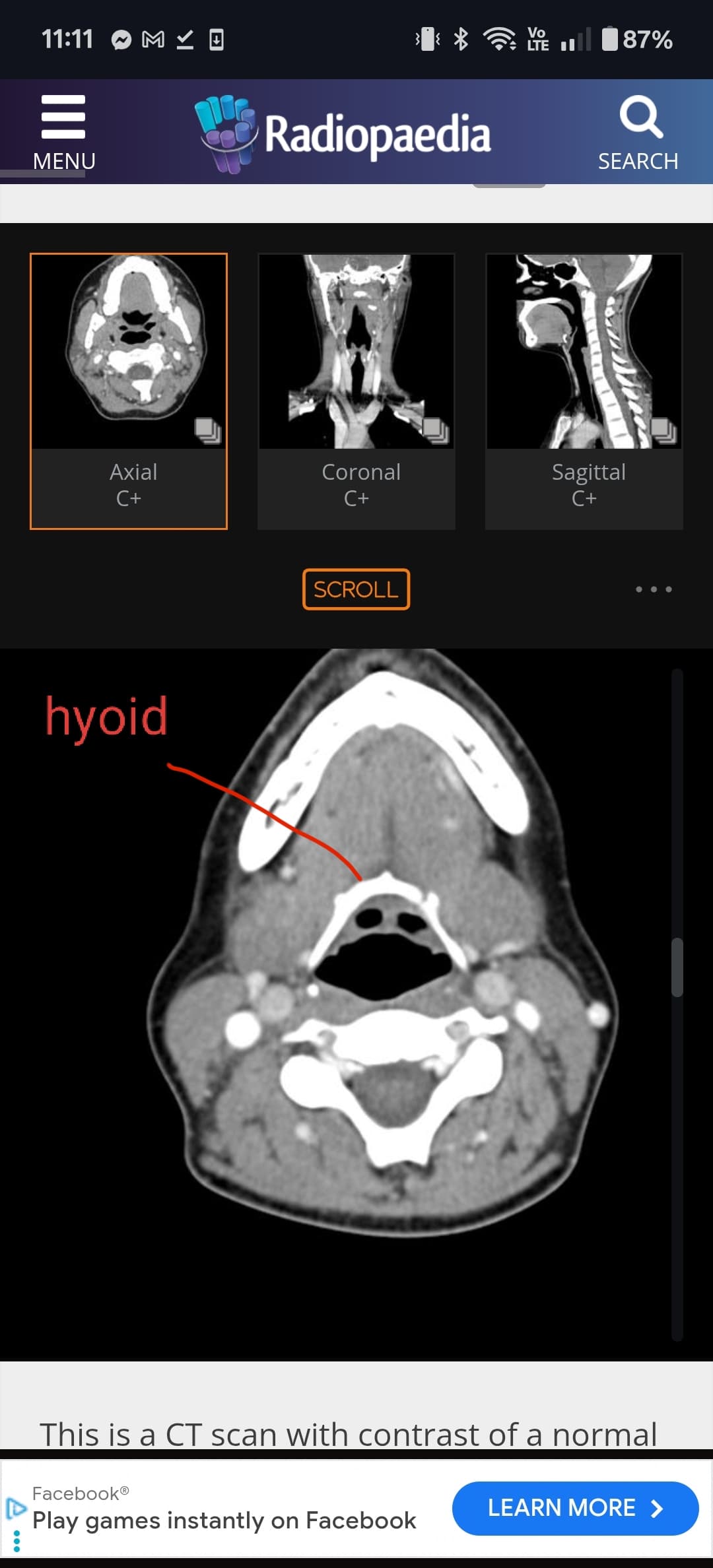







@TexasEagleSuffer see annotated image attached.
Your right greater horn is in contact with your right carotid bifurcation. Your left greater horn is in very close proximity to your cervical spine. I suspect the right greater horn is causing most of the symptoms, especially if your hyperacusis and pulsatile tinnitus is worse in your right ear.
