Hi everyone, I’m posting again (I posted back in May) as my symptoms have slowly become more noticeable and I’ve started to join the dots to other things that I’m wondering might be related to my elongated styloids that have been around for a number of years.
I’d welcome any advice.
Background: I saw Mr. Axon via an NHS referral in 2019, and I specifically recall during my consultation, while he was viewing the scan slices looking down through the top of the head/throat, that he said, in terms of the transverse process styloid, on the left-hand side the vein is not as big as the right—but that there is evidence that there is a bit of narrowing at that point on the scan.
I’d thought I’d only gotten my scans on a disk but my husband found the data on our computer so I have my 2018 scans but I’ve regressed in my computer skills - and can’t seem to be able to work out how to look again at what Mr Axon was seeing during the meeting. I’d very much welcome any advice on what my scans show in terms of vascular issues.
Connecting the dots
I’m realising that I may have had subtle, long-term symptoms that I never connected to my neck or the styloids until now. I’m wondering if these are positional/vascular issues now that I look back:
Hair-Drying (Long-term): When I position my head to the left to dry my hair, there’s a specific neck movement that causes momentary vision loss and I quickly adjust to regain vision. I can’t reproduce it and I stopped tilting my head that way during hairdrying, to avoid it.
Exercise Intolerance (Long-term): Any activity more strenuous than chores /gardening and walking, consistently makes me feel ill and run down for the next few days. I’m wondering if this could also be related. I had thought up until now that it was Post-exertional malaise (PEM).
Other possible links
Coughing Dizziness: When I cough a lot, I get severely dizzy.
Swallowing Dizziness: If I drink a beverage quickly I get really dizzy/lightheaded.
Pain in the last few months:
Soreness - Feels like something rubbing against something inside the throat, mainly on the right side.
stabbing nerve pain on the left side when my head is at specific angles.
Pulsating Tinnitus: Static, pulsating tinnitus in my left ear that worsens with the throat pain that has been ongoing for the last month or so.
I’m asking my GP for a referral back to Mr. Patrick Axon.
(If denied referral to Axon): I’m going to request a referral for a Dynamic CT/MR Angiography (CTA/MRA) with positional views to see if there’s mechanical/vascular compression.
Hi! Lots of your symptoms sound like they could be related to ES, some sound like IJV compression- pulsatile tinnitus is often caused by that, but the vision loss with head position & maybe the coughing dizziness could be artery compression…Obviously the soreness in your throat & swallowing/ coughing can be more classic ES symptoms, & stabbing nerve pain could be the trigeminal, facial or glossopharyngeal nerves depending where you get the pain?
I hope that you get a referral to Mr Axon, he does like scans done his own way as you probably know, so if you do get a referral then best to wait before getting any scans done. If you don’t, then the scans you want to get done would be useful, but it might be worth also getting images of the venous phase too, in case there is IJV compression, it sounds from your consultation like there might’ve been from your previous consultation…
Are you able to upload your images on here?
@SKC100 swallowing causing dizzinesss has me a bit worried that you may have something going on with the greater horns of your hyoid bone or the superior horns of your thyroid with respect to your carotid arteries. Swallowing should not move the styloid, and thus, IJV compression (if caused by styloids) should not worsen when swallowing - therefore something else may be going on and I tend to lean towards the carotid arteries when movements like that cause directly cause dizziness.
If you want, I suggest putting your CT files from your 2018 scan into a folder on google drive and then private messaging me a link to the folder. That way I can download your imaging onto my computer and go through the entirety of the imaging (and construct 3D models as well). You would no longer be anonymous to me, but I would be keeping your personal information private. Let me know your thoughts!
I will add though that swallowing could move a pocket of calcified stylohyoid ligament if it’s separate from the styloid because it’ll move with the moving ligament. But you’d still want to assess whether pockets of calcifications are located close too carotids.
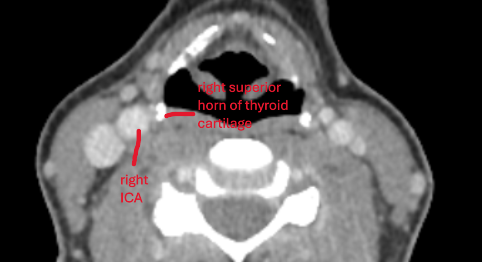
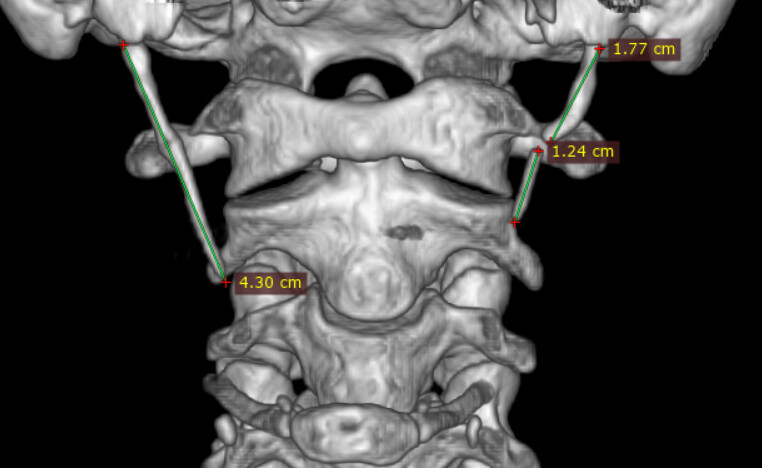
I had the opportunity to view @SKC100 ‘s CT imaging. See attached annotated images.
Between the skull-base and C1, both of your IJVs are compressed by your styloids. It is hard to see your left IJV as it is your non-dominant (or smaller) IJV.
At the level of C1, your right IJV become wedged/compressed between your right styloid and C1. On your left side, your left IJV is being compressed solely by C1 at this level. However, your left styloid at this level is in direct contact with your left ICA.
At the bottome end of C1 / upper end of C2, your right styloid makes contact with your right ICA.
Further down, at the level of the thyroid cartilage, your left superior horn is in very close proximity to your left ICA.
I have also attached 3D image showing your continuous elongated right styloid and your left normal length styloid that is followed by a pocket of calcified stylohyoid ligament.
Research shows that any styloid that is within 3mm of a carotid artery increases the risk of stroke. Both of your styloids (well, right styloid, and left calicified pocket of stylohyoid ligament) is in direct contact with your ICAs. This is stylocarotid syndrome. I high suggest getting the styloids/stylohyoid ligaments removed, and as close to the base as possible. This will remove any bone contact with ICAs and will allow the IJVs to open up between the skull base and C1.
Reminder that I am not a doctor nor radiologist. Hope this helps!
A massive thank you to TML. Your time and expertise in reviewing my 2018 CT data is genuinely appreciated, and I cannot express my gratitude enough. Your analysis is terrifying, but essential.
I’m currently overwhelmed with information and preparing for my GP appointment this Friday
The Measurement Question: My old report suggested a length of 8cm on the right, but TML measured the bony process at 4.3cm. I understand that the contact risk is now the critical issue, not the measurement, but the difference is causing me some anxiety about the accuracy. Is this difference just due to measuring the ligament vs. the bone itself?
Seeking Advice for the GP Appointment (Friday): My primary goal is to get an urgent, direct referral back to Mr. Patrick Axon at Addenbrooke’s. Given that Mr. Axon focuses on venous outflow, how should I best frame this conversation with the GP?
* Should I present TML’s findings as a “Second Opinion from a private consultant” and insist the GP must act on the confirmed ICA contact and stroke risk?
* Does anyone have advice on how to successfully push for the Dynamic CTA/MRA scans (with positional views) to prove the arterial compression in motion?
* Are there any other specialised surgeons or neurovascular specialists (in the UK) I should ask to be referred to at this stage, just in case?
Any advice on navigating this urgent step is greatly appreciated. Thank you all for the invaluable support.
I suggest forgetting about the lengths of styloid /stylohyoid calcification all together. The length does not matter. The fact of the matter is that on both sides the bony structures are in direct contact with your ICAs. Doesn’t matter what the lengths are. The eagle syndrome definition of needing to be over 3cm is way out dated and surgeons know it. So long as the styloid/stylohyoid ligament is long enough to reach vascukar structures, they have the potential to cause symptoms. The difference in measurements are likely just software related.
This is how I would frame things to your GP: “I have been experiencing bouts of dizziness that are exaccerbated by swallowing and head movements. This imaging shows that my styloids and calcified stylohyoid ligaments are in direct contact with my ICAs. I suspect that they are causing ICA compression with the head movements and swallowing, or they are causing vasovagal responses. Either way, I would like to see Dr. Axon again, as I am concerned about stroke risk, and he is one of the only surgeons in the area with the expertise to remove these bony structures. Here is a couple of articles that explicitly state stroke risk due to styloid-carotid proximity. One study found that a distance of less than 3.9mm is identified as stroke risk, and I have direct contact on both sides when I am simply laying down on my back looking straight (i.e., CT standard suppine position). There is nothing else that can explain my dizziness, unless you have any other theories as to why head movements and swallowing could specifically cause my symptoms. I believe I have stylocarotid syndrome and would like to see Dr. Axon.” - something around those lines anyway. Any sane doctor would not turn their heads on this because then they would be responsible for a stroke if it ever were to occur. I will also mention that you are at stroke risk. The carotid arteries have strong walls, and it takes a lot of continuous mechanical irritation or a swift/strong compression movement to damage the wall. I would just be careful with any full range of motion / swift head movements until they are dealt with.
you do not need a dynamic CTA/MRA. It would be needless radiation exposure because we already know that your ICAs are in direct contact with your bony structures. There is literally nothing else to explain your symptoms. Dynamic imaging actually just risks getting false negative because there could be a fluke where the specific positions they ask you to be in for the imaging could actually be best for increasing the space between your ICAs and styloids. If you get false negative it’ll be harder to get doctors to take you seriously. (although I think most doctors will take you seriously with the current imaging you have, once they actually realize the extent to what is happening).
I will let @Jules help you on the specialists piece in the UK. Dr. Axon is discussed frequently, but I would think that there could be one or two other ES surgeons?
I just wanted to send a massive thank you for your latest detailed response and for framing the situation so clearly for me. It was exactly what I needed.
I truly appreciate you taking the time to provide the essential clinical articles and calming my anxiety around the immediate risk. It has been invaluable.
No worries!! Happy to help. Make sure to bring those articles (probably just the abstracts) to your GP. Providing them with evidence based research always helps!
Subject: Update: Thinking of moving forward privately with Mr. Axon / AI Data Analysis
Hi everyone,
I wanted to share an update on my situation. I am currently thinking of moving forward with a private consultation with Mr. Axon rather than continuing to wait on the NHS.
My referral was originally kicked off in November 2025, so I’ve already been in the system for about 18 weeks. Just a week ago, the “My Planned Care” dashboard showed a 23-week average, but the update on March 20th jumped that to 32 weeks (with 8 in 10 patients waiting 49 weeks). The goalposts essentially moved 9 weeks further away just as I was getting close, and I’m now looking at mid-to-late June at the earliest.
I’ve been using a chest strap monitor synced with video to track my triggers, and the AI analysis of my recent logs suggests a very specific “smoking gun”:
The AI Assessment: Based on the “switch-like” speed of my heart rate jumps—specifically an immediate +26 BPM spike (e.g., jumping from 43 to 69 BPM) in under 30 seconds while standing and dressing—the AI indicates this is highly likely Carotid Artery Syndrome (Vascular Eagle’s).
Mechanical Correlation: The AI flagged that these spikes correlate exactly with neck flexion and reaching (e.g., leaning over the sink or moving washing).
Vascular Indicators: It also noted that the dull ache in my right temple during these spikes matches the referred pain map for the carotid artery/plexus, which sits right next to my long styloid.
I’m sorry that the waiting time is so long, the NHS is crazy right now! It’s especially worrying when you have possible carotid artery irritation/ compression… Mr Axon does have criteria for ES symptoms and whether he’ll do surgery, more members have seen him for IJV compression as this is something he’s researched. @Warrick posted about that in this discussion: UK surgeons - General - Living with Eagle
But he’s a good surgeon, so worth seeing. We do also have another doctor we’ve been given the name of who has written a research paper : Mr Paul O’ Flynn , London - not done surgery for any of our members , but apparently trained Mr Hughes, and is an ENT / Skull base surgeon and has co-authored this research paper for VES: The Eagle Has Landed: an unusual case of Eagle’s syndrome - PMC
We’ve not heard of anyone who has had surgery with him though.
Hi @SKC100 I am waiting surgery with Mr Axon NHS for left styloidectomy and C1 resection. Have been on waiting list since Aug 2025, spoke to Addenbrookes on Fri and they said it would be around Aug/Sept 2026 for my surgery. I have also enquired with Nuffield & The Spire regarding private surgery with Mr Axon, Nuffield have quoted me £14,700. Still waiting for quote from The Spire, but just to let you know they told me they cannot offer surgery privately with Mr Axon until June.
@Rosie - I’m so sorry the wait for surgery via the NHS is sooooo L-O-N-G! How are you doing as you wait? Are your symptoms somewhat controlled or are you just plain miserable?
Hi @Isaiah_40_31 I’m doing ok, thank you. I had 8 months seeing an Osteopath who worked gently on my upper spine so that has relieved a lot of my neck pain and headaches and I am no longer having migraines, thank goodness. I still have the other symptoms ear pain/fullness, pain in the mastoid/back of skull, under the ear, constant pulsatile tinnitus. I think having the gentle Osteopath work has given me enough relief to manage the other symptoms with pain killers (Nefopam) and muscle relaxants. I also try not to sit to long as this definitely does not help. We plod on, its good to hear from you
I’m glad that you’ve found a few things to help you while you wait, and thanks for the info about prices…a bit worrying that even privately you’d still have a few months to wait! I hope that you can hold on until September