Hey everyone, it’s Buzz here.
I will aim to update this post with my case history, radiology images and videos, test results, findings, and timeline as I progress through my ES journey.
First off, I wanted to say hi and introduce myself.
I haven’t read all the posts on this forum yet, but I’ve been reading as much as possible over the past few months, absorbing all of the knowledge and advice that I can.
The people here are amazing - every question I’ve thought of, has been answered in another post. It’s been a long learning process, and I feel much more confident in my understanding of ES.
I’m so grateful for this community - I believe that it’s already saved me a ton of time, effort, and pain. I hope my own contributions can serve as thanks for this incredible resource.
It’s a pleasure to meet you all. Even though we haven’t met in person, I feel invested in your stories from reading through your years of suffering and success.
Reducing suffering is a great goal, and a community that helps each other to do that is a beautiful thing. I appreciate you all.
My own journey has been long and painful - decades of chronic symptoms. I’m a 40 yr old guy living in Sydney, Australia. I have a wonderful wife and family who have supported me through all of this beyond anything that I could have hoped for. I am truly blessed in that regard. Healthwise, life has been a struggle for decades. At this point I am debilitated and disabled to a significant degree. Thankfully, earlier this year, I made significant discoveries in my CT scans relating to abnormal TSPs, IJV stenosis and possible ES as the cause of my symptoms. I’ve gone from my lowest point in my life to feeling truly hopeful.
I’m getting a referral to see Dr Elliott here in Sydney, and it will probably be a few months until my first appointment with him.
I’ll start posting my case history, findings and radiology images below, and joining in the other discussions. I hope my story can one day become one of the many successes on this forum.
I have so many different radiology images from different scans, it’s hard to know what to upload.
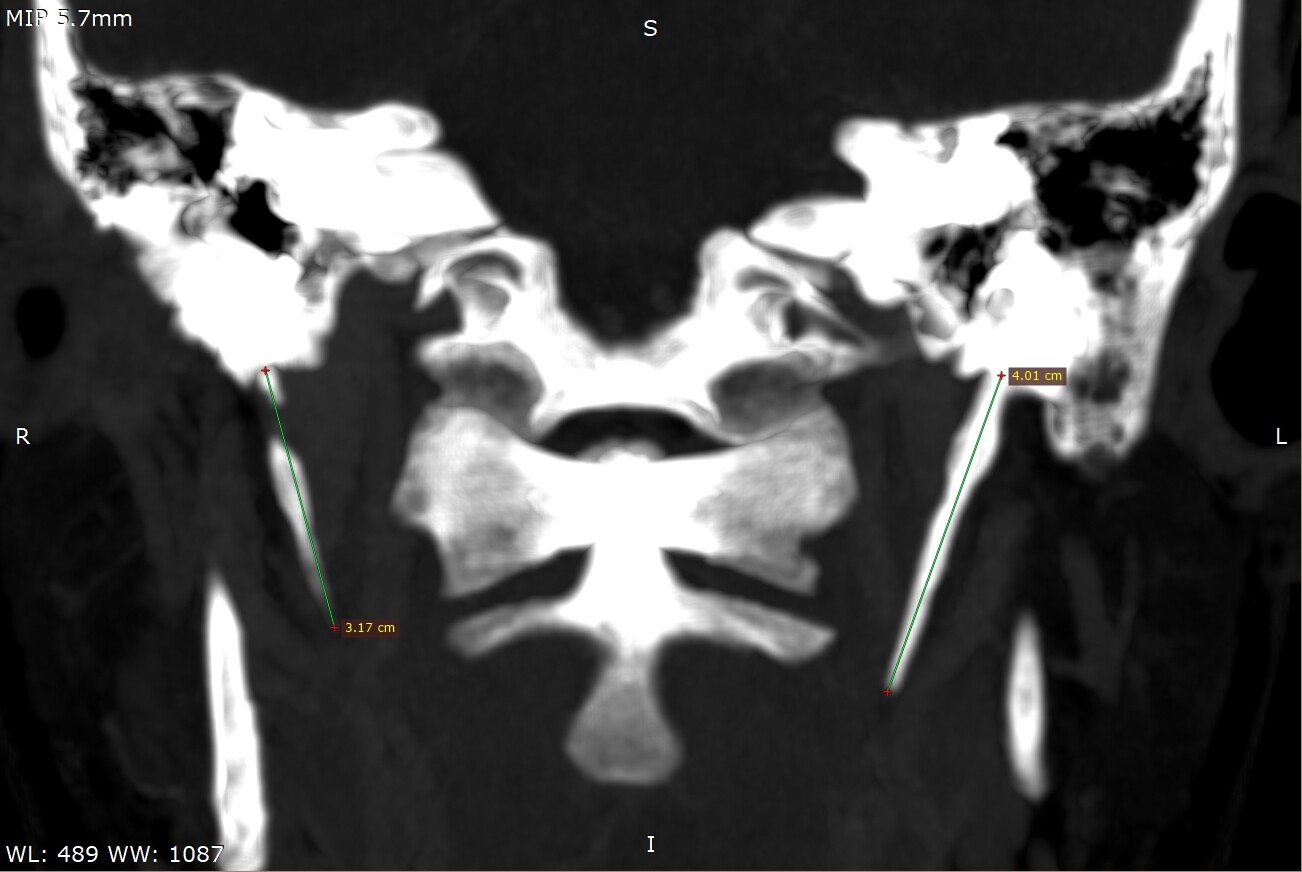
I’ll start with a CT slice of both of my TSPs:
Here is my left IJV:

Here is a video that I created using the software Radiant, it includes 3D reconstructions of my CT scans:
https://www.youtube.com/embed/S3WEDUuq1Cc?vq=hd1080
Please feel free to share any comments or insights that you have about these.
I’ll upload more later.
Thank you!







