Hey there. So I’m attaching a Pic of the C1 you mentioned ( I think this is it ). What are your thoughts?

@Ihurt can you go up or down until you can see the full C1 tranverse process? I’ve attached mine to show what I mean. Just want to see the full wings of your C1.

Okay, so I am attaching a few images. These are the only ones I have that are similar to yours. Can you see anything from these?





Besides Dr. Osborne, Dr. Cognetti will do a consult w/o anything other than the scan you’ve had done, @Ihurt, it’s just that he’s booked out till next Jan. or Feb. Most doctors now require their consults to be paid out of pocket by their patients i.e. they don’t accept insurance coverage for the consults. Knowing this would free you up to consult with whichever doctors you want to w/o concern about getting approval from your insurance. Having a diagnosis in hand would allow you to proceed to try to find help in your state or to know you need to do an appeal w/ your insurance company to see a doctor out of state. Health insurance companies have patient advocates on staff who is there to help patients with appeals to get coverage for non-covered medical care especially for rare illnesses or syndromes.
2 Likes
It looks like you right IJV is compressed. Hard to tell which spot the IJV is on the axial views without being able to scroll up and down in order to trace the vessels. Nevertheless, you do have right IJV compression. The short thick styloid is maybe part of the cause but other structures are probably also contributing to the compression. (C-1, nerves, artery, scar tissue/fascia)
4 Likes
Thank you for looking at the images. So I wonder how compressed it is, and is this the cause of my symptoms. I will need to figure out where to go next with this. I will likely have to find a specialist to send my scan to so they can look at it. Sad thing is, not many of the neurosurgeons will even give you a consult virtually unless you have a diagnosis with CTV. I might have to try sending them to Osborne, but not sure of his expertise in diagnosing or spotting different compressions. There is one neurosurgeon here Dr. Konstantin Slavin at University of Illinois, but I am sure I will need a referral. Not sure how much knowledge he has either. This is such a conundrum.
2 Likes
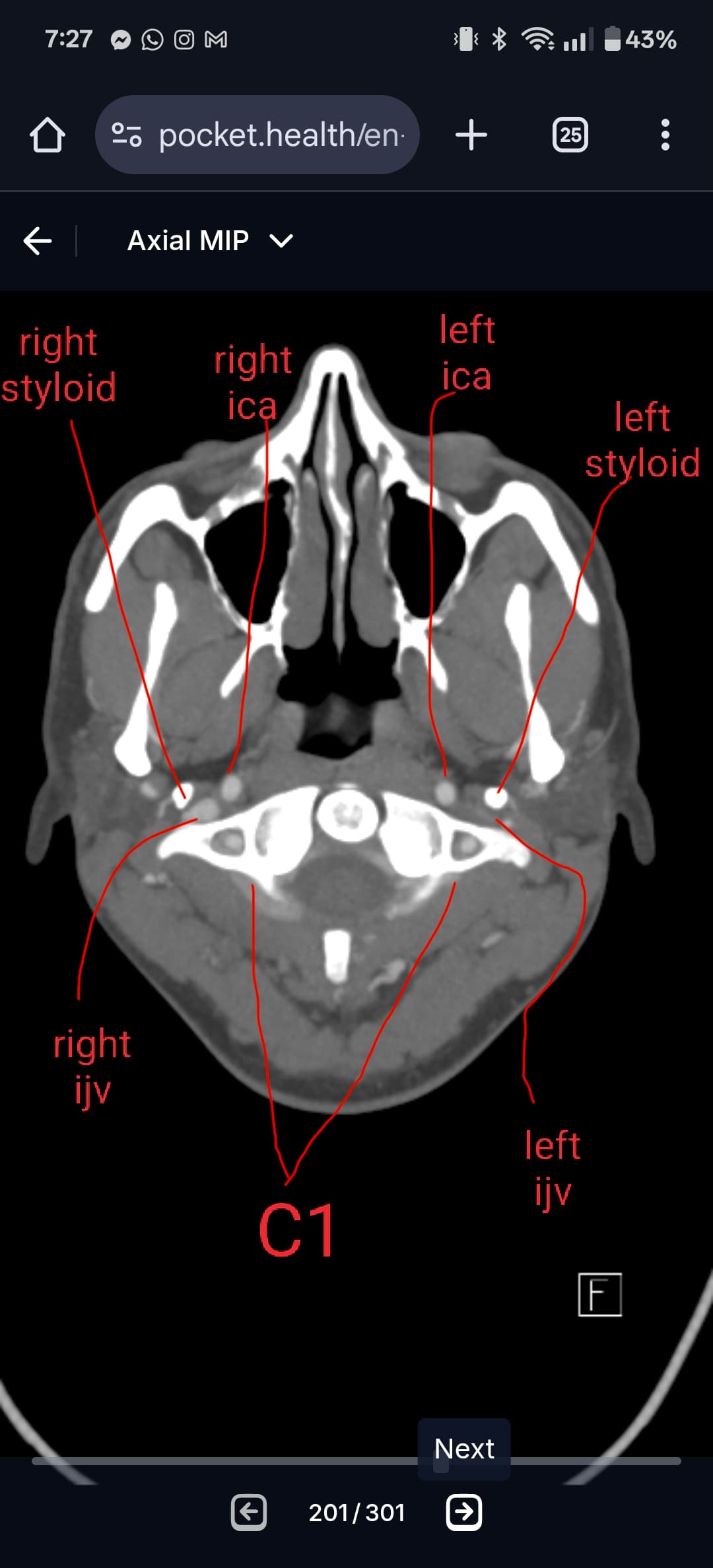
@Ihurt see attached your annotated imaging.
Looks like both your IJVs are compressed. But your right IJV looks worse. In this specific slice, it appears your right ijv (left side of image) is compressed between your styloid and C1, and may sort of be wrapping along the side of C1. This aligns with the 3D imaging you showed earlier with your right IJV. Like @Rex said, it’s sometimes hard to know which vascular structure is what without having the full imaging and being able to follow it. I’m usually quite good, but your right side is throwing me off, not sure if there’s a lack of contrast or things are super jumbled. I’ve attached my own imaging to help show you the landmarks to compare with your own. I highly suggest watching my tutorial on CT imaging for the axial view - just type “axial CT tutorial” in the forum and you’ll find it. It’s a ~15min video where I help you locate and follow vascular structures. I’m not a radiologist but I hope it can help.
Your left IJV has some compression, which looks to have only C1 involved (at least at this frame.
Whenever there is IJV compression there is likely vagus nerve compression/irritation as well.

2 Likes
Thx for your ever present help, @TML. You read the scans like the doctors do. ![]()
3 Likes
Thank you for looking at my images. I just wonder how much of this is causing my symptoms. I don’t have my symptoms daily, they come and go. My worst issue are headaches that affect the top of my head and back of my head ( occipital area). Was told it is likely migraine and neuralgia. I also have MCAS which I think also is contributing because certain foods can set my headaches off. However, movement of my head can too. I also have SVT heart palpitations which is definitely set off through movement at times. Those are my main issues. I do agree that the vagus nerve is likely being irritated. I just don’t understand why I can go periods of time with no issues. I definitely need one of the specialists out there to look at my CT images. Herein lies the problem because most of the neurosurgeons like Constantino and Dr. Peter nakjai will not even talk to anyone unless they have diagnosis and CTV. My friend found that out. She had to get a CTV first to see Nakjai as well as an MRI/ MRA to see Constantino with only a virtual appointment and only then will they look at her images. Her primary care was able to order her the CTV because her CT clearly showed severe compressions. The specialist i saw here ( Dr. Stepan office) she is an ENT head and neck surgeon, she said all was normal. Who knows if she even looked at the images. That makes it almost impossible for me to get a CTV ordered. My insurance would flat out deny coverage. Any ideas how I should move forward? I mean there is one neurosurgeon here in Chicago at University of Illinois Dr. Slavin. I am not even sure how good he is or not. Also I would definitely need a referral to even get in to see him because you can’t normally just see a neurosurgeon without a valid reason. They like doctor’s to refer patients. I probably could get my primary care doctor to refer me ( maybe). Then there is the question of is surgery the right thing? I’ve read not so good things about having the C1 messed with. Then there is the risk of making matters worse because scar tissue and adhesion can develop after any surgery and this can make matters worse in the end. ![]()
2 Likes
@Ihurt What scans did you have taken? It looks like you have had a head and CT with contrast. Did they do a scan without contrast first? That means you would of had a CT of the head and neck with and with out contrast. Did they hook you up to a machine (mechanical pump) that injected the contrast and then time your scan or was the contrast injected by hand and syringe?
A CTA is a CT scan that is taken after a pump that infuses the contrast and is timed (phased) to capture the contrast in the ateries and major arterial heart vessels. Then a second scan (delayed phase) is timed to capture the contrast in the venous system after the contrast has mainly passed out of the arterial side. So normally to see the CTV a CTA is ordered and captures both the phases.
So a CT with contrast that is injected by hand normally captures mainly the venous side depending on how fast the technician takes the scan after the contrast is injected. So a CT with contrast can be considered a CTV if it captured the needed vessels.
People, Dr’s, facilties all have different meaning and protocols for CT, CTw/wo, CTA, CVT, angiography.
Some people consider a CTA with delayed (venous)phase an angiogram. When I think of angiograms I think of catheter insertion with flouroscopy. Anyways it all confusing. I think your scan should be good enough have a consult and should quailfy as a CTV. Problem can arise talking to front office personal that do not get this. They require a CTV and you tell them you have a CT w/wo contrast and they reject you.
That happened to me dealing with Dr Nakija office. I had a CT w/wo contrast and they wanted a CTV. They could see everything that was needed on the scan that was provided. They wanted a CTV from the top of the head down to the clavicle. My scan shielded(block) the top 1-2 inches of the top of the cranium. So they wanted a new scan. My PCP ordered the CTA with delayed phase of head and neck. I sent it to them and they can came back saying it is not a CTV. I has to explain to them that it included both phases. That it had the CTA and the CTV on the disk. The new scan did not reveal anything that was not on the previous scan. Just jumping through the hoops and more radiation.
4 Likes
I’m sorry you had to go through that to “hack your way” into hopefully getting an appt w/ Dr. Nakaji @ Rex. It’s crazy how ignorant the front ofc staff is in some of the "super specialists offices. You’d think they’d be trained to know what the different scans are & how they’re done so they can both understand what’s needed & help patients understand it too.
Your explanation of CTA/CTV/angiogram, etc, is excellent. Thx for taking the time to spell all that out.
2 Likes
I had a CT of head and the whole neck with and without contrast. They took a picture first without any contrast. Then she came in and injected me with contrast and they took the picture afterwards. They had me tuck my chin down while taking the picture once the contrast was injected. As far as Dr.Nakija, my close friend has a virtual appointment with him. He wouldn’t even make an appointment with her until she had the CTV already done. She had already had other scans but he said it had to be a CTV of the whole head and neck down to the clavicle. He wouldn’t order it either because he said the only way he could order it is if my friend flew out there for an in person appointment. Because her CT had clearly shown elongated styloids and it also showed severe compression in her right IJV, she was able to have her primary care order her the CTV. My issue is that my styloids are not elongated, they are less than 1cm. My guess is the radiologist maybe wasn’t looking for anything else at that point? On my report it said all major arteries and veins are patent and Not obstructed. Not sure how they could even see that on a CT. So therein lies my issue, they are saying I do not have Eagle Syndrome based on my styloids being normal is my guess and that my symptoms are being caused by something else is what this doctor who ordered my CT said. I now have to hope to find a specialist who has knowledge about ES to at least read my scan more thoroughly. I mean there is Osborne who my friend told me will look at my scan and to a virtual consult with me. However, he is not a neurosurgeon so I’m not sure how much he will know seeing as my styloids are not even elongated which is what he mainly deals with. My insurance won’t cover out of Illinois either. Because my CT says all is good, that complicates my even being able to get another scan if needed. My insurance would likely deny it unless I can get another specialist here to agree something is wrong. There is one neurosurgeon here at University of Illinois, I think his name is Dr. Slavin. I have to do move research though to see if he is equipped to deal with this or what his level of expertise is with this. I might be able to get my primary care to refer me to him. I don’t need referrals to see specialists, but most neurosurgeons want patients to be referred by another doctor. I have to convince him that I need a second opinion on my scan. What a mess to say the least.
1 Like
Sorry to hear about the insurance issues.
You can try to take some key images you have to your PCP provider and show them what’s going on with the IJV compression. Explain to them that there is only 4-5 specialist that routinely treat this. Then explain that you need an order for MRI H&N with and with contrast along with a CTA H&N with delayed phase to get a consult with the specialist needed to treat the IJV compression. I think Dr C would be OK with the CT you already have and you would just need the MRI. Its hard advocating for vascular ES when most MD’s just don’t know about it.
4 Likes
Would you be able to research head & neck vascular surgeons otherwise in your area? I can understand your dilemma & not knowing where else to go…sometimes members have been able to get their scans re-read by radiologists with more experience, as we can all see compression of your IJVs- I think some members have used online radiologists? @vdm made a suggestion in this post:
Continuation from 2022 beginning with Appt with Hackman - General - Living with Eagle
3 Likes
I can try and see if I can get a virtual consult with Constantino. Not sure what an MRI will show though or if my insurance will even approve it. I also might try and look into seeing a neurosurgeon here who supposedly knows about ES to see if he can read my scan to see what he says. Thank you for the advice and response, I appreciate it.
3 Likes
@Ihurt - It wouldn’t be a standard MRI but an MRV you would need to get to show your IJV compression. I still also have some concern about the greater horns of your hyoid bone, but perhaps you need to focus on one thing at a time right now.
2 Likes
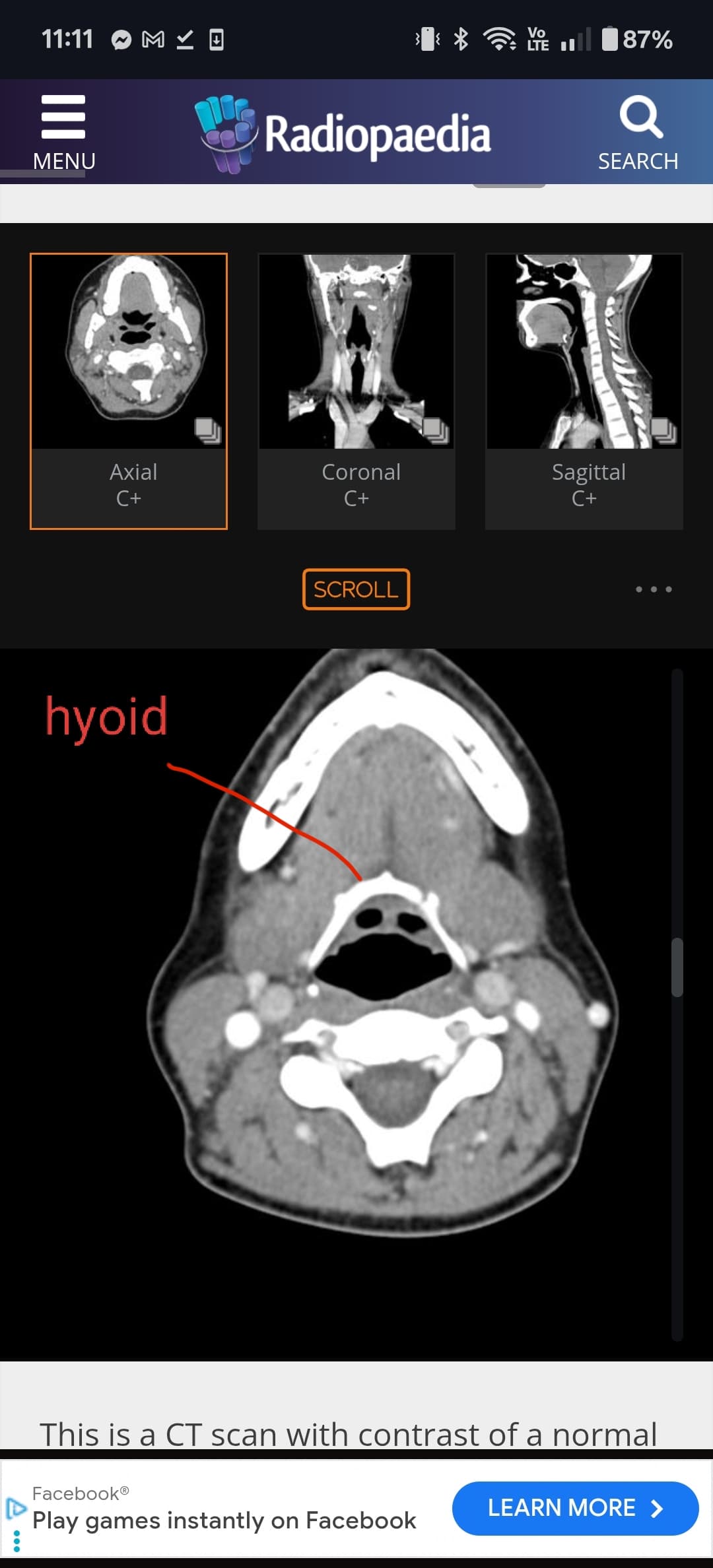
@Ihurt if you go back into the axial view I can help you locate the hyoid bone. I’ve attached some images to help you. Look for the horseshoe shaped bone. Depending on the angle of the bone, sometimes the whole bone is captured in one slice. Bur often times the tips of the greater horns are slightly higher up than the body or main front piece of the bone. The tips of the greater horns is the important piece, so make sure they are in frame.

1 Like
@Ihurt if you go back into the axial view I can help you locate the hyoid bone. I’ve attached some images to help you. Look for the horseshoe shaped bone. Depending on the angle of the bone, sometimes the whole bone is captured in one slice. Bur often times the tips of the greater horns are slightly higher up than the body or main front piece of the bone. The tips of the greater horns is the important piece, so make sure they are in frame.
I attached a few images of what I think show the hyoid bone. Can you see anything from these images?




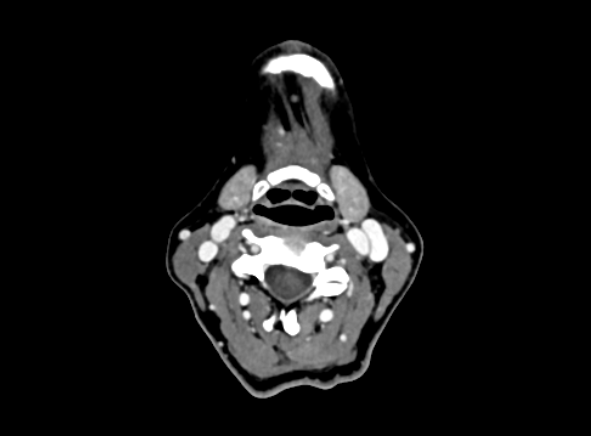
@Ihurt can you go up a slice or to in order to see the very tips of the bone? I’ve drew circles to show you where they should be roughly.
