I find what you’re saying (@KoolDude) extremely interesting. One of my NIR who was the one who found my bilateral IJVS said that from my cerebral angiogram / balloon angioplasty alone, along with my symptoms and CT and MRV imaging, a pressure reading would be an unnecessary step.
He mentioned something about it not being so accurate and something about blood flow turbulence effecting the results. He told me he can spend the time to explain it to me when I’m better and we have time and that if I really wanted it, we can do it but he didn’t think it was necessary for my case and wouldn’t change the plan or results.
I know many Drs would disagree with him, but I’m curious what he / you meant by the turbulence effecting the results.
I’m currently scheduled for bilateral styloidectomy with Dr Hackman.
Here are the angiogram procedure notes, apologies because it’s quite long.
Pre Operative diagnosis: Severe Intractable headaches that are worsened by straining without relief and worsening over the past two months and preventing the patient from working
Post Operative Diagnosis:
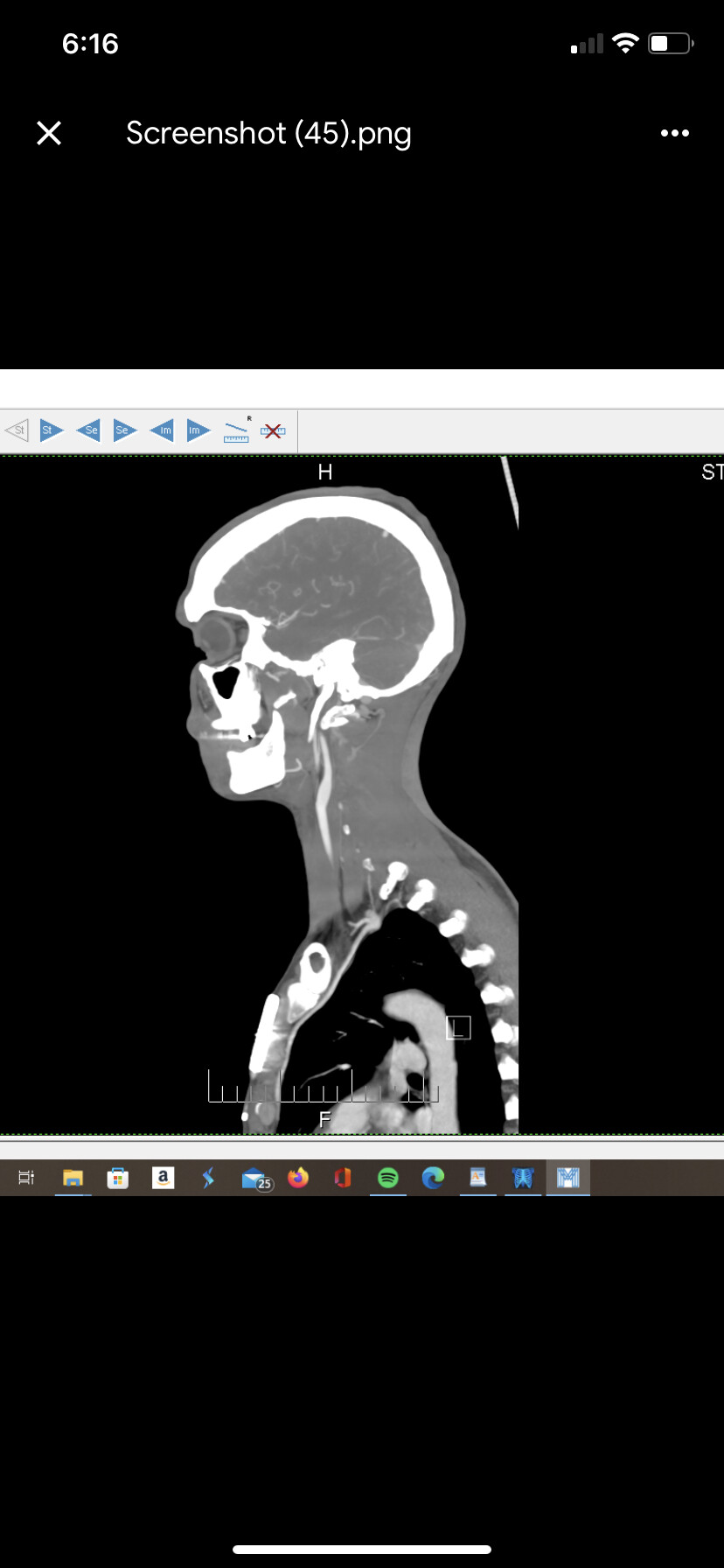
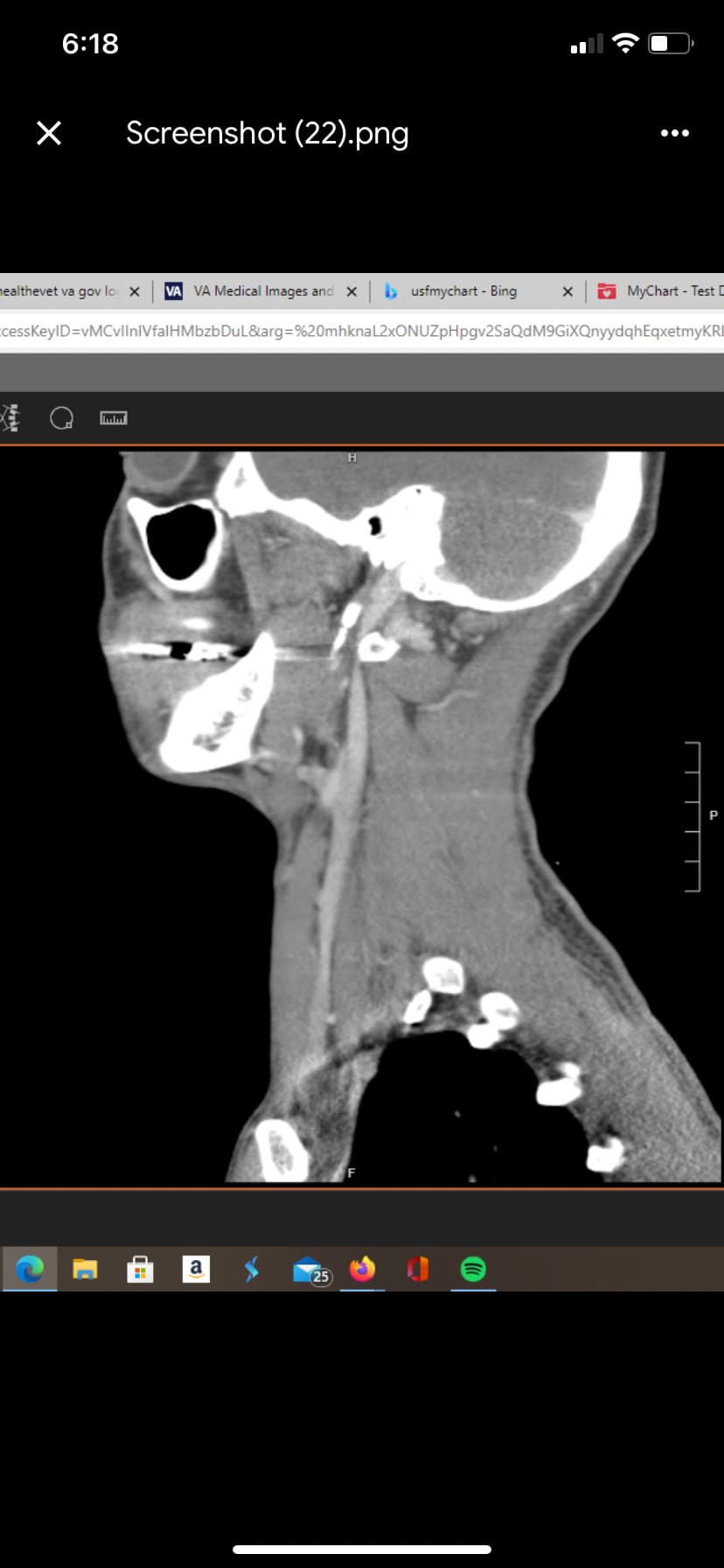
- Occlusion of the left internal jugular vein with severe stenosis of the right internal jugular vein which is worsened by neck extensison status post venous angioplasty with some improvement in venous congestion but persistent occlusion of the left internal jugular vein between the left styloid process and the left C1 transverse process.
Procedure :
- Diagnostic cerebral angiogram
- Diagnostic Venogram
- Venous Angioplasty
- Intravascular ultrasound
Anesthesia : General Anesthesia
Preoperative Medications : None
Introduction : A timeout procedure was documented, the patient’s name date of birth and medical record number as well as the procedures to be performed was confirmed by the entire team, after everyone in the room agreed, the procedure continued. After the patient was placed under anesthesia, both groins were prepped and draped in the usual sterile fashion.Using sterile Seldinger technique the right common femoral vein was punctured using a micropuncture kit. Over a 3mm J wire a Neuron max sheath was introduced into the vein and then hooked up to a continuous heparinized flush system.
Using sterile Seldinger technique the left common femoral artery was punctured using a micropuncture kit. Over a 3mm J wire a 5 French sheath was introduced into the artery and then hooked up to a continuous heparinized flush system.Via the sheath a 5 French diagnostic Catheter was introduced over a 0.35 Terumo glide wire, into the abdominal aorta, the catheter was then double flushed. The following vessels were than sequentially selected, and digital angiographic acquisitions were than obtained.
Vessels Selected :
The right common carotid artery was selected and injected with cervical views.
The right internal carotid artery was selected and injected with cranial views.
The right vertebral artery was selected and injected with cranial views.
The left common carotid artery was selected and injected with cervical views.
The left internal carotid artery was selected and injected with cranial views.
The left vertebral artery was selected and injected with cranial views.
Follow up angiograms were obtained
3D dyna CT was performed
Diagnostic Imaging Findings :
The right common carotid artery was selected and injected with cervical views.
The right common carotid artery appears normal without any areas of irregularity or stenosis.
The right external carotid artery appears normal without any areas of irregularity or stenosis.
The right internal carotid artery appears normal without any areas of irregularity or stenosis.
The right internal jugular vein appears larger with stenosis at the level of the right C1 transverse process.
There is prominence of the right external jugular vein.
The left IJV is not clearly visualized.
The right internal carotid artery was selected and injected with cranial views.
The right internal carotid artery appears normal without any areas of irregularity or stenosis.
The right middle cerebral artery appears normal without any areas of irregularity or stenosis.
The right anterior cerebral artery appears normal without any areas of irregularity or stenosis.
There is filling of the posterior circulation via the pcom.
There appears to be some venous congestion.
There is a severe stenosis of the right internal jugular vein at the level of the C1 transverse process.
The right vertebral artery was selected and injected with cranial views.
The right vertebral artery appears normal without any areas of irregularity or stenosis.
The right PICA appears normal without any areas of irregularity or stenosis.
The basilar artery is faintly visualized due to its connection with a proximal PICA branch.
There is flash filling of the PCA’s
There is venous congestion with delayed emptying via the dural sinuses.
The left common carotid artery was selected and injected with cervical views.
The left common carotid artery appears normal without any areas of irregularity or stenosis.
The left external carotid artery appears normal without any areas of irregularity or stenosis.
The left internal carotid artery appears normal without any areas of irregularity or stenosis.
The right internal jugular vein appears larger with stenosis at the level of the right C1 transverse process.
There is prominence of the right external jugular vein.
The left IJV is occluded at the level of the left C1 transverse process. Venous collaterals are noted in the same area.
There is prominence of the left external jugular vein.
The left internal carotid artery was selected and injected with cranial views.
The left internal carotid artery appears normal without any areas of irregularity or stenosis.
The left middle cerebral artery appears normal without any areas of irregularity or stenosis.
The left anterior cerebral artery appears normal without any areas of irregularity or stenosis.
There is filling of the posterior circulation via the PCOM.
There again appears to be some venous congestion.
The left vertebral artery was selected and injected with cranial views.
The left vertebral artery appears normal without any areas of irregularity or stenosis.
The basilar artery appears normal without any areas of irregularity or stenosis.
The left PICA appears normal without any areas of irregularity or stenosis.
The right PCA is visualized and appears normal.
There appears to be some venous congestion.
INTERVENTION:
The neuron max catheter was navigated into the right internal jugular vein.
IVUS:The refinity catheter was navigated into the superior sagittal sinus and pull back was initiated.
Superior Sagittal Sinus: No significant stenosis
Torcula: No significant stenosis
Right transverse sinus: No significant stenosis
Right Sigmoid sinus: No significant stenosis
Right Internal Jugular Vein: Severe stenosis at the level of the C1 transverse process.
Venous Angioplasty:
A viatrac 6 mm x 20 mm balloon was navigated over the wire and postioned across the stenosis in the Right IJV.
It was inflated to a pressure of 10 atm and pulled back gently.
There was a significant deflection of the balloon suggesting hypermobility in the region.
The balloon was then deflated and removed.
The left internal jugular vein was then selected and the neuron max catheter was navigated into it.
A synchro wire was navigated into the IJV but could not go past the occlusion in the left IJV despite multiple attempts including using the microcatheter and different microwires.
IVUS:
The ivus catheter was navigated into the left IJV and pullback was initiated.
Left IJV: No significant stenosis
Left Brachicephalic vein: Moderate stenosis
A decision was made to try and pass the occlusion from a superior approach using the right IJV.
The neuron max catheter was navigated into the right IJV.
A transform 4 mm x 20 mm balloon was navigated over a wire past the torcula into the right sigmoid sinus.
The microwire was then able to cross the left IJV occlusion relatively easily.
The transform catheter was able to after a few attempts, cross the occlusion. The balloon of the transform catheter was inflated and then deflated.
It was then brought proximal to the occlusion and a check injection was performed and it showed no improvement in the occlusion.
3D Dyna CT:
3-D rotational Dyna CT was also performed. All source images from the 3-D rotational acquisition were sent to a dedicated workstation for reconstruction and review that was performed personally by myself.
The dyna ct confirmed that the left IJV occlusion was at the site of the left c1 transverse process against the styloid process.
Follow up Angiogram 1:
The right common carotid artery was selected and injected with cervical and cranial views.
The right common carotid artery appears normal without any areas of irregularity or stenosis.
The right external carotid artery appears normal without any areas of irregularity or stenosis.
The right internal carotid artery appears normal without any areas of irregularity or stenosis.
The right middle cerebral artery appears normal without any areas of irregularity or stenosis.
The right anterior cerebral artery appears normal without any areas of irregularity or stenosis.
There is filling of the posterior circulation via the pcom.
There appears to be some venous congestion.
The right internal jugular vein appears larger with stenosis at the level of the right C1 transverse process.
There is prominence of the right external jugular vein.
The left IJV is not clearly visualized.
Follow up Angiogram 2:
The left common carotid artery was selected and injected with cervical and cranial views.
The left common carotid artery appears normal without any areas of irregularity or stenosis.
The left external carotid artery appears normal without any areas of irregularity or stenosis.
The left internal carotid artery appears normal without any areas of irregularity or stenosis.
The left middle cerebral artery appears normal without any areas of irregularity or stenosis.
The left anterior cerebral artery appears normal without any areas of irregularity or stenosis.
There is filling of the posterior circulation via the PCOM.
There again appears to be some venous congestion.
The right internal jugular vein appears larger with stenosis at the level of the right C1 transverse process.
There is prominence of the right external jugular vein.
The left IJV is occluded at the level of the left C1 transverse process. Venous collaterals are noted in the same area.
There is prominence of the left external jugular vein.
Follow up angiogram 3:
The left vertebral artery was selected and injected with cranial views.
The left vertebral artery appears normal without any areas of irregularity or stenosis.
The basilar artery appears normal without any areas of irregularity or stenosis.
The left PICA appears normal without any areas of irregularity or stenosis.
The right PCA is visualized and appears normal.
There appears to be some venous congestion.
The neuron max and diagnostic catheter were removed.
Conclusion : Hemostasis was obtained using an 5F mynx closure device for the arterial site and manual compression for the venous access site. The patient tolerated the procedure well and there were no complications.
Intraoperative Medications : None
Materials Utilized : Diagnostic Angiography kit
Rest as above
Impression :
- Occlusion of the left internal jugular vein with severe stenosis of the right internal jugular vein which is worsened by neck extensison status post venous angioplasty with some improvement in venous congestion but persistent occlusion of the left internal jugular vein between the left styloid process and the left C1 transverse process.