Hi. Newbie, so please bear with me. I’ve been leaking CSF for a few years, with 5 blood patches to date. I get terrible “Rebound High Pressure”/Intercranial Hypertension when I’m patched. But often when I feel pressure, if I take Imitrex/Sumatriptan, it helps. My neurosurgeon and 2 neurologists have both told me if the Imitrex helped, then it was a migraine, and not RHP/IH. I’m finding it a little hard to believe I’m having this many migraines again – I had nerve decompression for Occipital Neuralgia in ‘22 and that took me from 30 migraines a month to about 8-10, so I know what daily migraines are like! I know Imitrex works, at least in part, by dilating blood vessels. Now that I know I have compressions on both sides (some smart folks here say both carotid and jugular may be involved), I’m wondering if Imitrex has been helping me because its opening up my blood vessels somehow?
Hey Tara,
My name is Merl I’m a member of the modsupport team here on Ben’s Friends.
I don’t have Eagles, but I’ve had lots of issues with IH (and neurosurgeons). I find it a little disconcerting when they come across with black/white type answers ie ‘…it’s either migraine OR IH…’. It’s never been black/white for me, there’s always areas of grey.
I was told the triptan family of meds were the miracle med for headaches… Not for me they weren’t. It seems there is a fair range of differing triptans and it can take a bit of trial and error to find the right fit for each patient. For me, I think the blood vessels played a part, but their impact was only part of the bigger issue.
Migraines/headaches are notoriously difficult to pinpoint cause/effect and yet some medicos often give us definitive type answers. I’ve given up on getting ‘answers’. I manage the best way I can for today.
So what do they believe is causing your CSF leaks if not high intracranial pressure?! And what’s causing the high pressure? If the migraine meds dilate blood vessels, then your theory is sensible, as others have found similar medications can sometimes help with the high pressure symptoms. Stick to your guns, & keep looking into the vascular ES diagnosis
Thanks so much for this Merl. I agree 100% that the meds (and doctors) are a lot of trial and error. I’ve been so lucky that the triptans work well for me. I’ve have Ubrelvy and Nurtec and others but I still go to Imitrex as my first line of defense. I also LOVE Ajovy, but the injections only work about 2 weeks for me and then I have a little withdrawal period. My neuro lets me take it every 3 weeks instead of 4, but I wish i could do every 2 weeks!
I would SO love to have a long convo with a group of smart neuros in the same room discussing/debating my weird noggin’. But instead we get the quick, automated response it seems.
I wish I could get someone to say what is causing my leaks or IIH! Dr. Schievink, one of the world’s leading experts on CSF leaks, is “not convinced” I even have a leak because he can’t see one on the (extensive, and invasive) imaging they’ve done. I haven’t sent the imaging for a second opinion because so far, the blood patches work to “cure” my leak symptoms, until the patch blows and the leak symptoms are back.
Schievink doesn’t believe in the spiky-leaky theory. I was all excited last year and brought a printed copy of that preprint study from Stanford to my appointment with Schievink – I had it all marked up and was like, “This is me!” He was totally dismissive and doesn’t think it’s legit. He’s also not convinced jugular compression has anything to do with CSF leaks. Womp womp. But I’ve learned he likes a lot of scientific evidence before he buys in, which I understand. I just need a more “think outside the box” kind of approach, since my body is always the outlier/rare case. If I had a dollar for every time a doc said to me, “Hmmmm, that’s interesting . . . .”
I’m sorry to say it like this, but, this is REALLY common. As one neuro said to me “I’m the surgeon, I’ve completed years of study, so I know. You? you’re just the patient you wouldn’t know…” I wanted to rip his damn head off. Arrogant sod. I was having these weird symptoms and was told “Well that just can’t be happening…” But it was and my symptoms were continually being minimised. Every dr, every specialist seemed to have their own theory/diagnosis and were very quick in dismissing/minimising any contradictory theory.
In your previous post you called it ‘IH’, in this post you call it ‘IIH’. Personally, I hate the whole idiopathic theory. For many years I was told 'There’s nothing wrong… …we think it’s all in your head…" little did I know just how real that would become. It was easier to label me “Crazier than a box of frogs” than to actually investigate. So, I ignored it all. Then one day I’m driving down the road and the lights went out. I couldn’t see and this made them investigate a bit more. They came out with the line “Ohh, look what we found…” Like it was all something new. I wanted to scream. I’d been telling them for years/decades, but nobody was listening. Then they came out with the label “idiopathic” and that lit my fuse . They found a little nasty growing in my head, but then wanted to call it all idiopathic The surgeons view was “Well, I operated. I fixed” so now there was no cause anymore, so it must be idiopathic. But the surgery had sent my whole system for a spin and they wanted to call it all idiopathic? GGGrrrrr. It’s like the medicos were saying “Well, just don’t blame me”
You know your body better than anybody, don’t let them discredit you. They make out they know all about it… … they don’t. They may know what their university textbooks tell them, but we’re not all listed in their textbooks. They like us to fit their diagnostic boxes, but when we don’t fit they can be very quick to dismiss or minimise our concerns. For them, standing on the outside, that’s easy. But for us, the patient, that minimisation only increases our stress levels.
Just know, you’re not alone in this. In other words “Me too”.
@tkk - I’m sorry I don’t remember if you have listened to these seminars or if anyone has posted the links for you but they contain substantial information about vascular outflow obstruction symptoms & causes that could be very helpful for you. I know of several people who’ve seen Dr. Schievink w/o getting any real help. It’s really rough when a doctor of reknown is so set in what (s)he thinks that there is not flexibility or willingness to continue learning or consideration of outliers.
We just had a zoom appointment with Dr Hepworth of Colorado today. We understood him to explain the leaks as coming from IIH that is caused by the overload of blood in the brain that comes from IJV compression not allowing the “waste” blood to leave the brain fast enough.
Just last Saturday we listened to the 2025 CSF Leak Conference. They had a lot of convincing facts about how rarely the “testing” that exists actually shows up a leak–especially if the leak has been going on for any length of time. Here is the link for their site. I thought there was going to be video available from the conference, but so far it does not look like they have posted this years up yet.
Your syptoms sound a lot like our daughters. Dr. Hepworth says hers is not so much styloid processes as it is a horny growth on her occipital bone that is compressing her IJV against the styloid.
Thanks for sharing this! Does Dr Hepworth feel he could do surgery to help her?
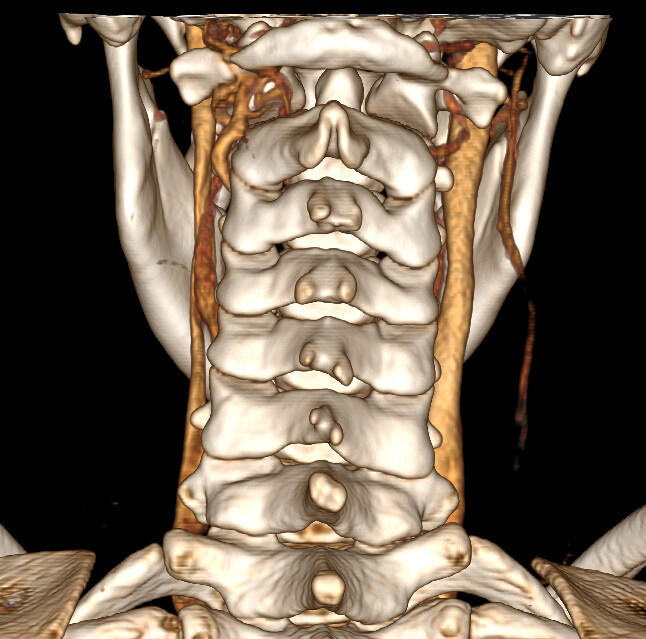
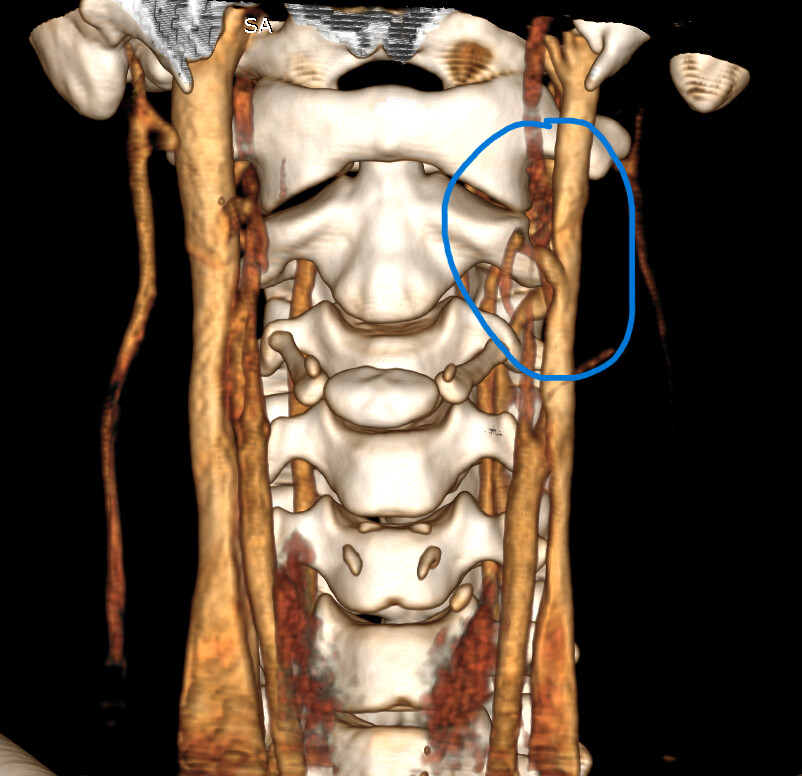
Do you have any imaging to share, it would be interesting to see that, but not to worry if it’s a hassle for you!
Those “extra” vessels are likely collateral veins that have developed to help offload the “old” blood from the brain in the absence of full IJV efficiency. Collateral veins are small veins that previously had a very minor role but take on a more significant function when the IJVs become compressed. The collaterals themselves can cause occipital pain & pain in the back of the head when they become engorged as they try to help the IJVs.
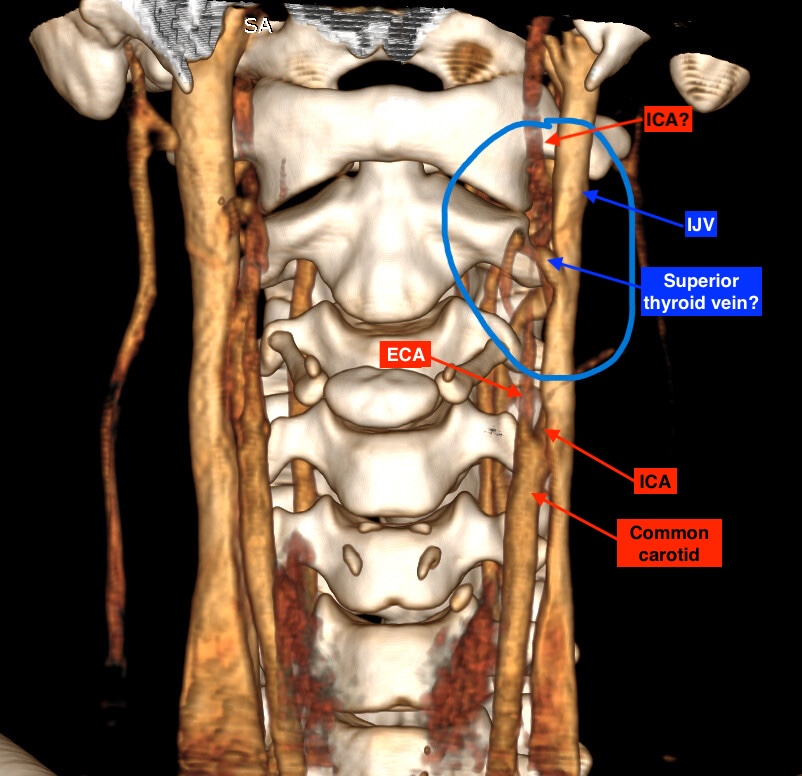
The vessels I can identify in the middle picture are the IJV + partial ICA & partial ECA & common carotid. It’s difficult to trace what’s what in the image.