From @suenami21 -
So my daughter had her icp monitoring done two days ago. They kept her at Hopkins until this evening and the results have not been officially given although they said that the fluctuations in her head pressure were not enough to consider it a problem with her csf so that is a good thing. Her pressure did rise significantly whenever she bent over or when her head went below her heart. Now we are left with the real possibility that the pressure has been coming from her jugular vein compression all along. We have a telecall with Dr. Costantino in early March so hopefully he will be able to look at her imaging and confirm that she does have compression at the C1 level. I’m not sure that her styloids are part of the equation but I think it is clear from the imaging that the C1 is involved. I’m going to upload many of her images that I was able to make into 3d with RadiAnt but I’m not sure how good they are. I would appreciate anyone who can view them to give me their opinion on anything they may see that could be causing her head pressure. I did include some 2D images as well because they do seem to show the C1 compression of the jugular.












Welcome, @suenami21!
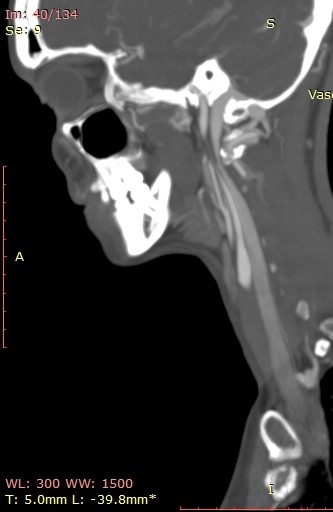
I’ve annotated a couple of the images you posted & will explain what I see under each image.

On the left side, your daughter’s IJV looks compressed at the styloid/skullbase level, possibly at C1 then lower between C4-C6. Because her cervical spine is so straight, it almost appears the transverse processes of those 3 vertebrae are in contact with her IJV & even below them. She has quite a number of collateral veins in the area of her skull base which is an indication of IJV compression. Though I can’t see the very tip of the greater horn of her hyoid bone on this side, it almost looks like it could be in contact with her external carotid artery (ECA) which can cause different symptoms than the IJVs.

There are very similar situations with the right side though I can’t see enough of the hyoid bone on this side to comment about the right greater horn.
Her compression doesn’t look severe, but since she’s symptomatic, the compression is enough for her body to be reacting to it. That Hopkins confirmed its not high enough to be a problem is good & bad. Good because she’s at lower risk for a CSF leak, but bad because I feel, in some respect, they were saying IH isn’t causing her symptoms which it most likely is.
Dr. Costantino does IJV decompressions that aren’t associated with styloid elongation so it’s good that you have an upcoming appointment with him for your daughter.
@Isaiah_40_31 has been thorough as usual with her explanation & labelling, I agree that there’s compression at the C1 level & also lower down, so I would ask Dr Costantino about both those areas when you see him; it could be a blood vessel or soft tissue otherwise further down in your daughter’s neck…
Good you have an appointment and scans to show Dr C, I hope he can help her!
Thank you so much for looking at these scans and for pointing out the possible issues and labeling them so well. The details really help. I can say that her vascular surgeon, Dr. Khanjan Nagarsheth at the University of Maryland Medical Center has scheduled her for a jugular vein decompression surgery in mid March. He did a venogram of her jugulars and found that both sides are 97% compressed around the C5-C6 level. She had a fusion in this area in 2021 and he believes the veins are being compressed by scar tissue probably from that surgery. He said he thought there was going to be compression around the C1 area as well due to the cta images but he didn’t find this to be true during the venogram. I am not convinced that there is no compression there so we decided to continue to find other docs who focus on any neck compression issues that could be present. Isaiah_40_31 I also am concerned about the neuro docs at Hopkins saying her mmhg pressures were of no concern because of some of the high numbers that were recorded when she was bending over especially. They were well above what is normal for people who are exercising but they were only concerned about certain aspects of the recordings. They did acknowledge that they believe her when she describes her head pressure etc but they were only checking for potential csf leaks if I’m understanding them correctly. We’re glad that is off the table but it bothers me that they don’t know what is causing it and so far have not figured out what the next step should be to figure it out. I am convinced it is compression in her neck and skull base. Some of the drs have said they think that that could be the case but dont want to say anything definite. Dr. Nagarsheth is doing one side and then the other 6 months apart and may possibly need to put a stent in her vein. We would like to avoid that since he said he would be putting her on a strong blood thinner and she would not be able to come off of it for a year. So we are hoping that Dr. Costantino will see compression issues that he wants to address and we may have to postpone her surgery with Dr. Nagarsheth if Costantino can do all of what may need to be done. Add her wedding to the end of April and there’s alot going on right now. Dr. Nagarsheth said she has alot of large collateral veins which tells him this has been going on for quite awhile. Isaiah_40_31 I find it interesting that you are spot on with the collaterals as well as the compression between the C4-C6 area. That must be what he found in the venogram. Do her styloids appear to be wider than what I normally see on diagrams? They don’t appear to be very long but maybe the width is a problem in her case
That sounds like a good possibility. I reread an older post today where it was mentioned that for patients who tend to develop a lot of scar tissue, Dr. Aghayev in Turkey puts a layer of fat around the IJVs after decompressing them to help protect them from future compression by scar tissue. Dr. Hepworth uses sheep tissue to accomplish the same purpose. That’s to say that there are things that can be done during surgery to help protect the IJVs from re-compressing post op.
Based on my experience of 11 years on this forum, if a person is suffering from the symptoms we know go along w/ IJV compression, then I feel like diagnosis based on manometry readings from a venogram alone are not an adequate judge. I’m also not convinced that simply checking mmHg pressures in the IJVs can determine whether there are CSF leaks or not. It doesn’t necessarily need to be astronomically high to cause a CSF leak as there is variability in tissue thickness & strength in the brain in each person. There are sometimes obvious external symptoms such as clear fluid that drains from the nose or down the back of the throat or from the ear(s) intermittently. This fluid tastes salty & metallic. Does your daughter experience anything like that?
I agree with your conviction. It sounds like the doctors at Hopkins don’t know as much about the relationship between IH & vascular outflow obstruction as they should.
I understand why your daughter may need a stent, but I also hope she won’t need one.
I think it’s an excellent idea that you’re getting a second opinion.
Her styloids are very wide at the skull base & are not very well defined. I think that’s why her IJVs looked compressed to me right at the styloid/skull base junction, but you’ll need to see what Dr. Costantino thinks.
I agree that her styloids do look pretty chunky at the skull base, so it’s worth seeing what Dr C says, but be prepared for the compression further down to still be an issue? Stenting should be a last resort I felt personally, I’ve been very lucky that my IJVs opened up enough after surgery to resolve the head pressure…
So sorry I have been mia after you so kindly answered my questions. I’ve been working on wedding stuff every chance I get. I did see your comment about postponing the wedding but unfortunately the venue and other vendors have been paid and the money is non refundable. So we are going through with it. Her telecall with Dr. Costantino was rescheduled from 3/4 to 3/18 unfortunately because her surgery with the vascular surgeon to clear the scar tissue compression at c5-6 was scheduled for today. We contacted the surgeon and discussed our concerns about what might happen if it was later discovered she has additional compression at c1 if he did his surgery now and he agreed that we should speak with Dr. Costantino first. Therefore, we pushed today’s surgery to 5/22. We may or may not keep that date depending on what Dr. Costantino finds. Unfortunately her condition seems to get worse by the week. The weather/barometer changes we are experiencing are creating havoc with her head pressure. I worry that we will speak with Dr. Costantino and he will say he sees nothing and then we’re back at square one. My daughter has disclosed that she often feels like she’s choking on her own saliva. That usually happens when the pain begins under her jawline which I think is the glossopharyngeal nerve perhaps? Correct me if I’m wrong. She has also noticed that when she turns her head to either side, but more so the right side to look behind her somewhat, that the whooshing sound increases and the throbbing also increases. I still remain hopeful that this is going to resolved, and I hope sooner than later. It gets hard some days to see the light at the end of the tunnel.
May I ask what your head pressure was like? She describes hers as having the worst nonstop sinus pressure all over her head that you can imagine. It never stops. Is it also true that people who had their tonsils out seem to have some type of compression at a later date? She had hers out when she was around 10. She is now 38.
Tonsillectomy is a known cause of ES, but not everyone who has that surgery goes on to have ES, and vascular ES is less common too… My head pressure felt like my head was being squeezed, & sort of felt buzzing, when it was really bad I would get a sort of sucking/ rolling feeling, like by brain was being rolled up, that was awful. Luckily mine wouldn’t be so bad at the start of the day (once I started sleeping propped up), but would build through the day & got horrible by the evening.
Choking on saliva does seem to be a common symptom- having too much saliva or the opposite, a dry mouth happen quite a bit. The choking sensation can be from the glossophayngeal nerve or possible the vagus nerve . Although pain along the jaw line can also be trigeminal nerve- they’re all commonly affected by ES.
It sounds like the compression gets worse turning her head, & that’s why she gets the whooshing pulsatile tinnitus worse the- mine was made worse with exertion & laying down, didn’t get worse with head turning, but the pain certainly did!
I’m sorry that she’s had to delay surgeries, but it does seem sensible to have a consult with Dr Costantino & get his opinion…
@suenami21 - I totally understand your daughter’s reasons for not delaying her wedding & actually suspected that might be the case. I know some venues require reservations a year prior to the event so cancelling is not an option unless one wants to start over or go elsewhere.
I’m glad your daughter’s appt w/ Dr. Costantino is still this month. With her symptoms being as severe as they are, I highly doubt he’ll tell you he sees nothing. I am glad her vascular surgery was able to be postponed until after your appt. w/ Dr. C.
Another option affecting her swallowing besides the GPN, & something that can contribute to IJV compression, is her posterior digastric muscle. It’s innervated by the facial nerve which is one of the cranial nerves most often irritated by elongated styloids thus if her facial nerve is “unhappy” it could be causing posterior digastric dysfunction. The digastric muscle is a key player in swallowing.
Weather/barometric changes are notorious for causing symptoms to worsen both for our vES & ES members. Many of our female members also notice symptoms worsen pre-menstrually & menstrually.
As @Jules mentioned, head certain head positions can cause symptoms to worsen so it would be ideal if your daughter could try to avoid turning her head to the right & practice turning her whole body to the right when she needs to look that direction. Is she sleeping w/ head/shoulder elevation at night, & has she tried icing her neck or using moist heat on it several times a day for 15-20 min at a time? There are gel packs that are meant to be frozen or heated. These usually come w/ a cover which can be moistened when using the pack for heat & used on the neck that way. Another thing your daughter can try are OTC lidocaine (5%) patches on her neck. They also come in Rx strength which is 10% lidocaine. One other thing that has helped a number of our members who have IJV compression is taking a blood thinner. I think we’ve mentioned that to you before. Is that something she’s looked into?
I hope your daughter’s appt on 3/18 provides her with answers & hope. Please let us know how it goes. ![]()
![]()
We finally have some answers. Today my daughter and I spoke with Dr. Costantino and he went through her 2d scans with us and given her symptoms and history, he has suggested that the next step is to get a test balloon venogram. He has referred her to another doctor for this procedure as he does not do this test himself. He said that she has what is called jugular vein outflow obstruction. This involves compression by the c1 transverse process but does not involve the styloid process as far as he can tell. He said this particular type of venogram will tell him if the compression is causing her head pressure etc due to the nature of how it is performed. If it is causing the pressure, he wants to do a decompression by taking the c1 tp away. He also does not think she has any compression at the c5-c6 level from scar tissue so he said in his opinion he does not believe she needs that surgery. That being said, I don’t think he has seen any of the 3d images which may support the compression in that area. I saw the venogram that she had and it shows the compression is at c5-c6. So we will have to revisit this with her vascular surgeon at some point. Dr. C did say that stenting there before alleviating the upper compression would potentially cause additional problems so it’s good we decided to wait to get that surgery until after we spoke with him. He said we can get her venogram done as soon as it can be scheduled and then he wants to get her into surgery if need be as soon as possible after she returns from her honeymoon. He said he is pretty confident that the balloon venogram is going to show significant compression that will require surgery. He also gave us a link to a fairly new video he created and posted to youtube that is called Internal Jugular Vein Decompression: Anatomy, Indications, and Surgical Procedure which I just watched. Here is the link for anyone who may be interested. https://www.youtube.com/watch?v=1xFzBp0oHwA
Thank you for posting the link!
It’s hard when you get two conflicting opinions (about the C5-C6 compression), but stenting I agree shouldn’t be rushed into & a good idea to get any other compression sorted first…Frustrating to need more testing but it’s good to get as much info as possible before making surgery decisions, I hope that you can get the venogram arranged soon ![]()
We’ve had other members also diagnosed w/ jugular outflow obstruction by Dr. Costantino. I’m glad he doesn’t think your daughter’s styloids are a problem as that will require one less step in her surgery. It sounds like she has a reasonable path forward at this moment.
I hope the balloon venogram gives the evidence that surgery will help her. I agree whole-heartedly that you should challenge his denial of the C5-6 compression since it’s been noted & is even visible on the images you posted here. Seems like Dr. C should revisit that as it would be good for your daughter to get all compressive forces dealt with in one surgery.
I hope & pray that her wedding is everything she’s planned & hoped for & that post honeymoon her IJV (s) can be decompressed & she can start feeling better & living her life more fully. ![]()
Thank you for your kind words for my daughter. The wedding is 5 weeks from Saturday and we are praying for the best. Dr. C is aware of her wedding and honeymoon so everything will be planned around that. She and I are both relieved by his call and explanation. Just getting that confirmation that you’re not crazy and there is a real physical cause for the symptoms you are experiencing. And we will definitely ask the doctor performing the balloon venogram to examine the entire jugular vein for any compression that may exist elsewhere. I would hope they will do that anyway but Ive learned to cover all bases when advocating for ones health. If he sees additional compression then I imagine Dr. C will revisit this and make the needed recommendations. I will be sure to discuss this with him no matter the venogram findings. Again, thank you for your support. This site is what saves me and her from feeling overwhelmed and completely alone with all of this. I should ask if it’s ok if I remain on here since at this point they are not technically saying she has Eagles Syndrome.
Yes it is hard. I believe she does have the c5-6 compression and hopefully the balloon venogram will show that it is there - will make sure the doc tests the entire jugular vein. If it shows up again then I’m going to make sure Dr. C addresses it as well. He was completely against a stent during an initial surgery which I am in agreement with. The risks of future complications are too great and should be avoided unless the jugular shows over time it cannot function without one. We should be able to get the venogram scheduled soon as there are openings in that docs schedule. It’s a matter of them getting the insurance approvals needed. He does fortunately participate in the National BlueCard PPO program which alows her to pay in network costs when receiving treatment out of state. We are 2.5 hrs away from Manhattan office or 3.5 away from the Sleepy Hollow office but either way it’s time well spent if it results in her feeling even 50% better at this point. But we hope for a near full recovery.
Of course you can stay here, jugular outflow obstruction is a cross-over with ES and we have members who have more C1 involvement than styloid and those with both so not strictly having ES doesn’t matter to us, it’s the same symptoms! We’re glad that you’ve found the site helpful and want to follow your daughter’s journey. Hope the insurance gets sorted soon for her venogram ![]()
@suenami21 - I second everything @Jules said. ![]()
So my daughter got married three weeks ago. She’s been back from their honeymoon for a week and we went to Lenox hill hospital today where she had another venogram of her jugulars this time with a balloon and an angiogram of the carotids. The good news is that she does not have any vascular issues in her head that are causing her symptoms. We do not have the official report, however the dr who performed the procedures said he did not see any pressure gradient issues however, she did go from a pain level of 8 to a 9 or 10 on both sides when he did the balloon test. He said he will review the data he collected in more detail and write the report but he can’t say if this is going to result in Dr Costantino performing surgery to fix the C1 compression. He said her blood flow looked good and he didn’t see any compression anywhere. He also said it is very unusual for a person to be able to feel the catheter going through the veins but she did and knew exactly where he had it positioned even before he announced where it was because it gives her pain. When I spoke with her after the procedure she told me that when he did the balloon in her left jugular she immediately felt a huge pain like a lightning bolt struck her on the left side of her head and made a very sharp pain. And the pressure increased all over. Then when he did the right side with the balloon she said she got a significant pain in the occipital area and it increased the whooshing sound tremendously plus tinnitus increased. The dr also said that because she’s dealing with such a high pain level already it’s hard for them to reproduce or increase her pain because it’s already so intense. But according to her it did increase her pain level and symptoms and she told him that as it was happening. We now have to wait for dr Costantino to look at the results and figure out our next step. We’re worried he’s going to say without pressure gradient changes her head pressure and all other symptoms are not being caused by her c1 compression that he pointed out in her cta scans. When we talked with him before he said he was certain she was going to get a positive result from the venogram. Does anyone know how Dr Costantino determines if surgery is warranted if the venogram is normal per the radiologist? Does he go by the symptoms that are documented over a long period of time plus the imaging he acknowledged shows compression? Any input is welcome.
@suenami21 I just want to say that I could also feeling the movement of the catheter inside my veins, especially as it went round past my ears. The movement itself didn’t cause pain, it was the release of the dye. The doctor said that usually indicates there is a migrainous quality to the sensation even though I have never had migraines. They tried me on an injectable migraine medication while I was waiting for my surgery date. It didn’t improve anything and the surgery improved nearly everything. I did, however, have significant pressure gradients across the C1/styloid compression. Wishing you and your daughter the best.
I’m glad that your daughter is married and had her honeymoon, what a start to married life for her though…it sounds horrible having the venogram & angiogram… I hope that Dr C will help your daughter despite no obvious pressure gradient issues ![]()