I recently saw an ENT due to my suspicion of ES. After I gave him a HD CT taken in 2014 and CTV taken in 2021, he told me that my styloids were a bit long and a bit over 3cm. I asked about the angle and to which he had no reply, and the thickness wasn’t spoken of. I wanted to add some images here to show the styloid and ask others non medical opinions. I suspected ES after a diagnosis of hEDS and its other comorbidities. The ENT said he could do a shot, and if it helped surgery would probably be the way.





@BirdsOfSore - Your styloids aren’t excessively long, but they’re pretty thick. They may be compressing your internal jugular vein on each side, too, though it’s hard to tell for sure from the angle of your imaging. Do you have any symptoms of vascular ES i.e. headaches, brain fog, visual changes, pulsatile tinnitus in your ears? If so, you will need to see a more specialized surgeon who will not only shorten your styloids but will also make sure your IJVs are decompressed.
This isn’t necessarily the best way to confirm whether surgery will help or not. For some people the injection (usually a mix of lidocaine & a steroid) does help stop symptoms for a brief period but for others it makes symptoms worse or does nothing at all. Because of the inconsistent results, it’s best to go by what your CT scan shows & what types of symptoms you have.
1 Like
Yes, I would say the vascular ES symptoms are more of a problem than the site local symptoms are. I also have signs of Intracranial hypertension on other imaging that include partially empty sella and extra csf in optic nerve sheaves and bulbous/tortuous optic nerve sheaves. I wasn’t too happy with the first ENT’s opinion, I might try Dr. Keith Sale at KUmed after I do more research on him. Dr. Hepworth seems worth the short trip to me as well.
1 Like
I agree with @Isaiah_40_31 , the styloids do look a bit long & definitely thick. It doesn’t look like there’s compression of the IJV between the styloids and the C1 processes, which is a common place for compression, it look like it could be higher up at the skull base, and difficult to see…
Dr Hepworth is very experienced with vascular ES, so if you can get an appointment with him then hopefully he’ll help you…
2 Likes
Should I take some images of where the veins enter the skull and transverse/segmoid sinuses? The original reason the CTV was taken, was because of suspicion of possibly transverse/segmoid sinus stenosis. I had a really good doctor from USC, whom then became head of neurovascular surgery at a hospital in Michigan; look at my images. He said there was mild to moderate stenosis in my transverse sinus area and also diagnosed me with hEDS and occult tethered cord. I had to travel to see him, we both thought that finding a neurosurgeon for OTC in my area would probably be ideal. I believe I do have a surgeon lined up for OTC release surgery in Chicago, but haven’t spoken in months. Now that I’ve found signs of ES, I am thinking that the styloidectomy is the least invasive of surgery options I’ve been offered and should probably be first before surgical approaches intradurally. As far as styloid and C1 causing stenosis, I feel like the side with my “Dominate” venous route can become compressed with head/body positions. That is just based off my perception of my symptoms tho.
2 Likes
@BirdsOfSore - Dr. Hepworth is an astute diagnostician & an excellent surgeon, however, he is booking surgeries in March now & initial consults in Feb. It can take patience & determination to get through to the office & not get stuck leaving a message on vm which might never get you a call back - just a heads up. If you can travel, Dr. Nakaji in Phoenix would also be a good option.
As far as the OTC goes, Dr. Petra Klinge in RI is the go to for that surgery, but I expect there are other competent surgeons who do the surgery who may be closer to you as you mentioned someone in Chicago.
1 Like
I’ve talked to Dr. Klinge via email and she is the one who recommended the surgeon in Chicago who was a former student of hers. Dr. Klinge is very impressive.
2 Likes
Good to know! I understand Dr. Klinge has health issues of her own & isn’t practicing full time so getting in to see her can be challenging.
I agree w/ you that starting w/ ES then working your way to more challenging surgeries is a good way to go.
2 Likes
You could send some images in the area you suggested. I’m not sure I can recognize problems w/in the skull though others may be able to. I think part of the challenge w/ the pictures you posted is that the top 2 & last one are zoomed in too far. Can you post them less zoomed in or other images from the side?
1 Like
That’s rotten, having those other surgeries to consider as well, but glad that you’ve had surgeons recommended for those… Sending you a hug ![]()
2 Likes






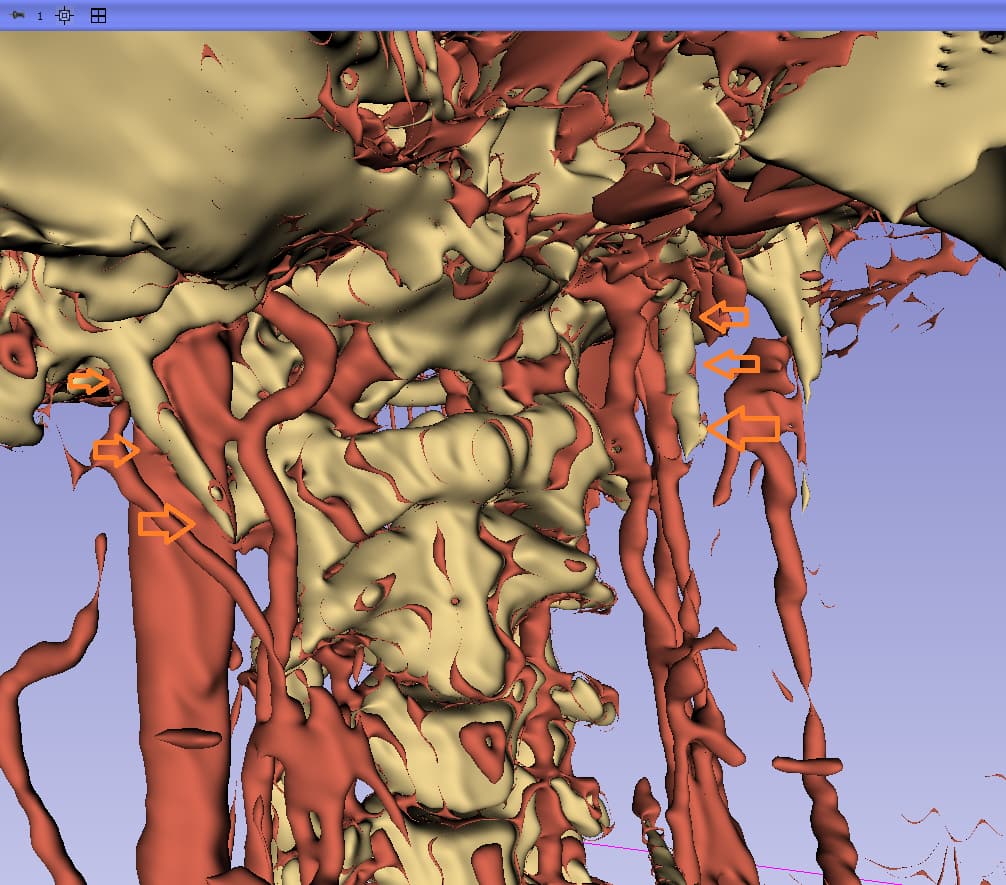
I’m sorry I can’t tell you anything regarding what’s happening inside your skull, but after some studying of your styloids & IJVs, it appears your right IJV is dominant & may have some compression between the styloid & skull base. Your left IJV is smaller/narrower & looks to be fine. However, I am not a doctor so please don’t take this as any sort of diagnosis.
I also observed that your cervical spine is fairly straight. We’ve noticed that many of our members have lost the natural lordotic curve in their cervical spine. The lack of that neck curve allows the styloids to come into closer contact with the nerves that create ES symptoms. It’s possible to restore the lordotic curve through gentle exercises but it takes some time. Our member @vdm posted some very helpful information on this topic: List of my favourite resources on YouTube to learn anatomy
I’ve annotated the image of your right styloid/IJV:

2 Likes
Hi , my name is Tammy.
My daughter has hEDS and had OTC surgery in RI with Dr. Klinge’s understudy Dr. Svokos in 3/24. Extremely successful.
I have ES and see Dr Katelyn Stepan from Northwestern in Chicago.
Considering surgery.
Who is your Chicago surgeon?
1 Like
Tammy,
Dr. Klinge got me in touch with Dr. Francesco Pucci at University of Illinois. He told me 50/50 anything would improve with surgery(I had seen Dr. Klinge’s data before this obviously.) I said I was happy with those Odds and he told me surgically 50/50 isn’t that great of an odd. I said I would still like to go ahead and he told me he would start the process of setting things up. That was the last I herd from him about 4 months ago.
Thank you for the reply,
I’d like to reply with some data that has helped find my ES diagnosis while searching.
Dr. Kenneth C. Liu (intracranial venous issues expert) (Diagnosed me with hEDS)
https://www.bronsonhealth.com/doctors/kenneth-liu/

And I’ve seen Dr. Pradeep Chopra’s name mentioned here once, he is at Brown University with Dr. Klinge and is in the pain management department. His lecture on hEDS/EDS and its comorbidities connected all the dots between hEDS/ES/OTC/POTS and other things.
")
I’m sure you probably have Dr. Klinge’s most recent paper in reguards to OTC, if not, here it is with video demonstration.
1 Like
That’s helpful info @BirdsOfSore , thank you for sharing that! Will you consider another surgeon if you don’t hear from Dr Pucci soon? Some members have asked to be put on a cancellation list and have got in quicker with doctors that way, might that be worth trying?
@BirdsOfSore - Many of our members have learned the hard way (by experience) that there are doctors’ offices who don’t follow through well so the burden of getting an appointment either in the office or for surgery falls on the patient. If you think Dr. Pucci is the surgeon you want to have do your ES surgery, then start calling his office once a week to check your status with their office i.e. where are you on their wait list or whatever type of list they keep of patients needing surgery & to whom Dr. Pucci has promised it. This is patient self advocacy & unfortunately it is becoming more common for each of us to advocate for ourselves to get what we need in order to have our health situations improve.
I also must say that it’s important for you to know how experienced Dr. Pucci is with ES surgeries. If he’s only done a few & since he’s only suggested a 50/50 chance of improvement, I’d highly recommend seeing a more experienced ES surgeon as the experienced surgeons have higher success rates than that.
I agree w/ @Jules. Thank you for the very interesting links.
1 Like
@Tammy1 - What good news to hear your daughter had successful surgery for OTC. I’m sorry she has hEDS though. I hope she is able to be more active & live her life more fully now that her OTC has been taken care of.
Since you’re considering surgery w/ Dr. Stepan you need to find out how experienced she is w/ ES surgeries & whether she uses the transoral (through the throat) or transcervical (through the neck) approach. Based on patient experience here, the transcervical approach gives better longterm results if the styloid is cut back as close to the skull base as possible which is more difficult via the transoral approach. It’s also safer because nerves & blood vessels can be visualized during surgery with the transcervical approach whereas w/ the transcervical the surgeon cannot see those things.
1 Like
I am still in the processes of trying to see Dr. Hepworth.
I did see Dr. Keith Sale last week, He told me my styloid was close to the jugular vein at the skull bass but he doesn’t do styloidectomies that high up, usually leaving around 2cm of the styloid. He recommend against a skull base surgery due to it being close to nerves and the jugular vein. He thought most if not all my symptoms were occult tether cord related more than eagles syndrome. He also mesured one of my styloids at 2.9cm while the other ENT had them both over 3cm.
I am trying to think of any tests Dr. Hepwroth might want done in advance of our appointment. Would anything like a jugular ultrasound be helpful?
Here is the note from Dr. Sale, I felt like he was avoiding the skull base for reasons I feel like it should be targeted.
Subjective:
The patient, with Ehlers-Danlos syndrome, presents with symptoms potentially related to Eagle syndrome. He was referred by his primary care doctor for evaluation of possible Eagle syndrome.
Since 2012, he has experienced recurring issues following an incident where he hit the back of his head and shoved his neck down. In 2014, he consulted an ENT due to persistent pressure in his head, and an HDCT of the sinuses was performed. Recently, he has been exploring the possibility of Eagle syndrome after being diagnosed with Ehlers-Danlos syndrome and consulting with a neurosurgeon in Michigan regarding possible occult tethered cord. Symptoms include a noise in his left ear with neck movement, pain throughout the throat, and sharp pains at the base of the neck. He also experiences pressure in the face and eyes, which he associates with increased intracranial pressure. He has not been able to work since 2015 due to these symptoms and spends a lot of time lying down.
He has researched and found that conditions like POTS and Eagle syndrome are common with Ehlers-Danlos syndrome. He has consulted with a neuro-ophthalmologist who noted signs of increased cerebrospinal fluid pressure, such as torsicity of the optic nerve and partially empty sella on imaging. He also has an arachnoid cyst.
He has been in contact with other individuals with Eagle syndrome and has noted that his styloids appear slightly long and possibly abnormal in angle and thickness, although not significantly longer than normal. He is seeking further evaluation to determine if his styloids have been damaged or re-ossified, potentially causing his symptoms.
Outside CT neck reviewed. Styloids measure 2.9cm on the right and 3.0cm on the left
Assessment and Plan:
Neck and throat discomfort
Symptoms since 2012 include cranial pressure, cervicalgia, and aural clicking. Imaging reveals styloid processes measuring 2.9 to 3 cm, which is normal. No significant vascular or structural compression in the neck. Eagle syndrome is unlikely the primary cause due to lack of significant anatomical abnormalities and its rarity. Surgical intervention is not recommended due to the normal styloid length and absence of clear neurovascular compression.
Occult Tethered Cord Syndrome
Diagnosed with Ehlers-Danlos Syndrome (EDS) and informed by a neurosurgeon about the possibility of occult tethered cord syndrome. Symptoms such as cervical and cranial pain and pressure may be attributed to this condition. Recommend follow up with Neurosurgery.
Total Time Today was 45 minutes in the following activities: Preparing to see the patient, Obtaining and/or reviewing separately obtained history, Performing a medically appropriate examination and/or evaluation, Counseling and educating the patient/family/caregiver, and Documenting clinical information in the electronic or other health record
2 Likes
I don’t know too much about OCTS, can it caused increased intra-cranial pressure? As you have obvious IH the something’s causing that…I don’t understand how he can say no significant vascular compression in the neck, from looking at your images ![]()
In respect to seeing Dr Hepworth, I personally wouldn’t worry about getting any more testing done as he’ll request any tests etc he wants and may well have a way he prefers, so best to wait. Although if anyone else who’s seen Dr Hepworth have input on that then please chip in!
2 Likes