Hi,
I uploaded my CTV scan into Radiant.
Clicked some buttons and was able to render these images.
Do they show IJV compression?
If yes, is it moderate or severe?
Compression from C1 or styloid or artery/muscle?
Thanks!!
Hi,
I uploaded my CTV scan into Radiant.
Clicked some buttons and was able to render these images.
Do they show IJV compression?
If yes, is it moderate or severe?
Compression from C1 or styloid or artery/muscle?
Thanks!!
@chrEagle really hard to draw any strong conclusions from the 3D models. The best view is the axial view.
If you want, I could take a look through the entirety of your imaging for you. Members typically put their CT files into a google drive folder and then private message me a link to the folder. That way I can download the imaging and go through it all. Let me know if this is something you’d be interested in. You’d no longer be anonymous to me, but I wouldn’t be sharing any of your personal information.
Thank you so much. Yes, I will put my images in a google drive folder – I have soft tissue and bone images. CTV neck with contrast from the TS junction to clavicle.
I will message you when images are uploaded. Thanks again!
I can’t see your styloids at all on those images, nor the C1 processes, so can’t comment, the IJVs look fairly full but it can look very different on the axial views as @TML says. I would say though that your neck looks like it’s lost it’s natural curve- aka military neck- which we see quite often. This could be contributing to a forward head posture which may make symptoms worse, or it could be it’s your body’s way of trying to open up the space in your neck, it’s one of those dilemmas we don’t know the answer too! But there are exercises which you could try in this post:
List of my favourite resources on YouTube to learn anatomy - General - Living with Eagle
@TML will hopefully look at your images down to your hyoid, it’s probably clearer in the axial view, but it looks like your hyoid might be against the IJV on your left side?
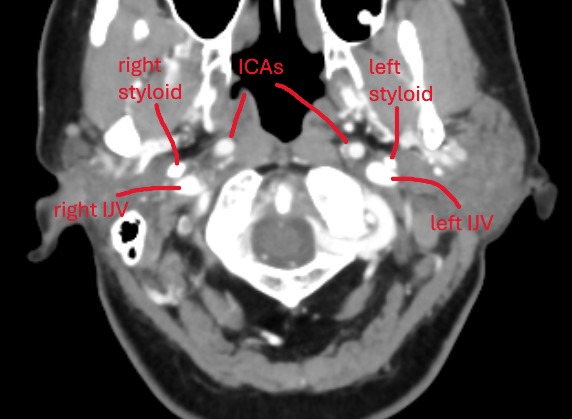
@chrEagle see attached annoted images (5 here of the axial view, and a 3D model in a following post)
Between the skull-base and C1, your left styloid comes in contact with your left IJV. Contact is normal, compression is not. I would be surprised if this contact is causing any symptoms.
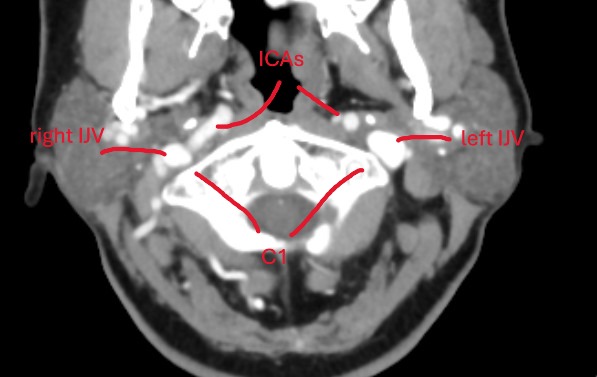
Further down, at the level of C1, there is some compression of your left IJV against C1. Neither styloids are contributing to any compression here.
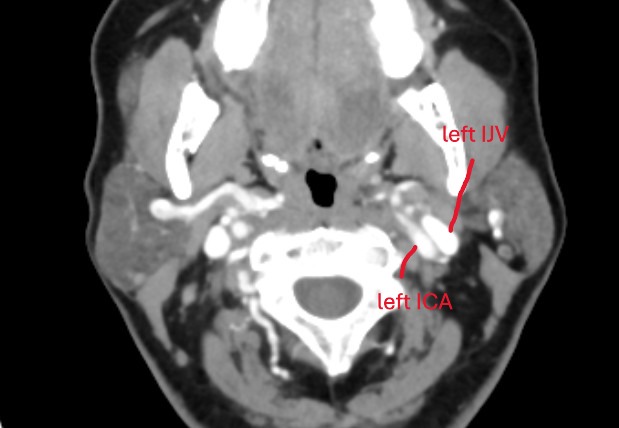
At the level of C2ish, your left IJV becomes compressed by your left ICA. Your ICAs are tortuous, in that they move from an anterior to posterior position and then go back to anterior position. On it’s way to to the posterior position, the left ICA compresses your left IJV.
There is no other IJV compression anywhere.
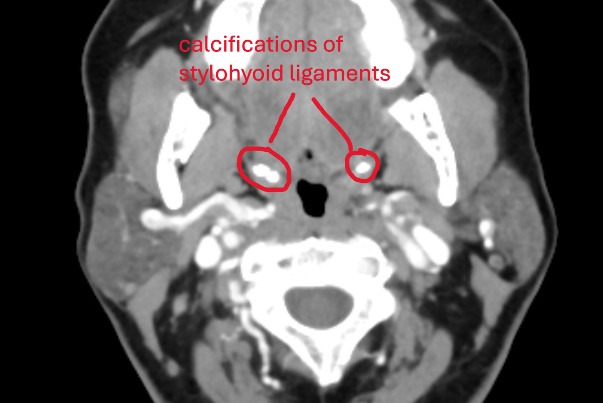
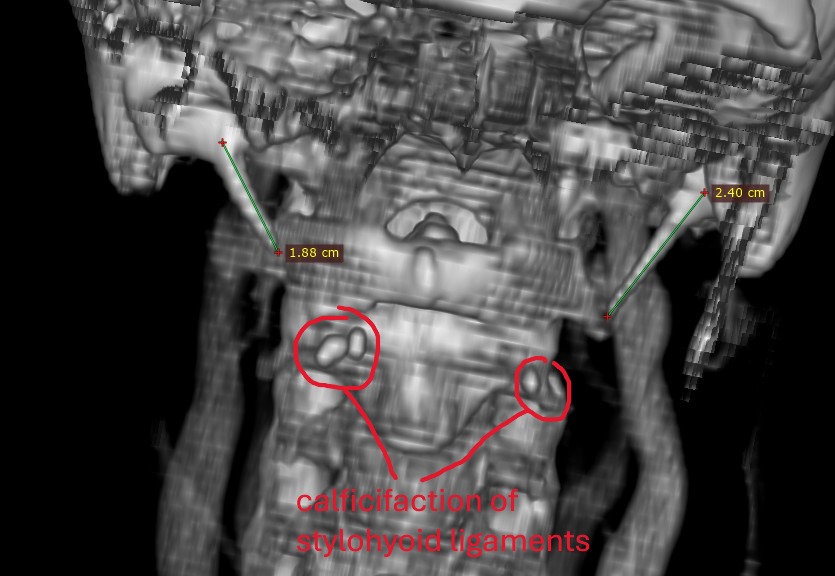
Further down, there is a pocket of calcified stylohyoid ligament on both sides. It may not look like much, but these little calcification pockets can irritated nerves.
Further down, your thyroid cartilage is in contact with you CCAs. This can commonly occur, but this positioning could cause symptoms when turning your head because the SCMs contract and could push the CCAs harder against the thyroid cartilage. Symptoms would most likely include pain the radiates up the sides of the neck and down into the top of the chest.
Just a reminder that I am not a doctor nor radiologist. Hope this helps.
@TML, Thanks so much for looking at my scans. Very helpful!
Is the left IJV compression by the left ICA moderate or severe? Can this cause symptoms? My jugular doppler did show very low velocities in the left IJV. I don’t have symptoms on the left.
I have pulsatile tinnitus on the right hand side with jugular doppler showing much higher velocities. Maybe contralateral flow from the blocked left side to right side is causing turbulence on the right and pulsatile tinnitus?
Thanks!
I can’t really comment on the severity of the IJV compression due to the ICA. The amount of IJV compression required to cause symptoms differs in everyone (which is why radiologists usually show no concern over IJV compression, even though they should because everyone is different). All I can say is that the diameter of your left IJV lessens when the ICA contacts it. Unless there is what I deam as “extreme” compression (e.g., styloid compresses IJV against C1 to a sliver) than it’s hard to say what’s moderate vs severe vs minimal. I think it’s possible that the left IJV compression by the ICA is capable of causing problems. A surgeon should be able to move the ICA so it’s course doesn’t interfere with the IJV.
I will add that IJV compression usually causes increased velocity (think about putting your thumb over the nozzle of a hose - the diameter of the opening is lessened but the speed the water comes out is faster), so it’s odd to me that your left IJV had lower velocities given the compression from the ICA. However, the upper half of your right IJV is smaller in diameter than your left IJV, which may explain why the velocity is faster in the right. Almost every CT I’ve seen had a dominant and non-dominant IJV.
There’s always the pesky jaw to consider as well. TMJ irritation can cause ear-related symptoms. So if you have jaw pain in the TMJ that should always be considered too.
@TML, Thanks!
Yes, the velocities in the left IJV are lowest just below the jugular bulb. The neuroradiology report also mentions that the belly of the digastric muscle effaces the IJV in this area. So, maybe there is soft tissue overcrowding in a tight C1-styloid corridor (you mentioned the styloid makes contact with the IJV here). This causes the IJV to collapse and the flow gets slower instead of accelerating as veins are low pressure systems unlike arteries – just my guess.
Velocities where the ICA effaces the IJV at C2 are normal so maybe that compression is not having an effect.
Was wondering if this overcrowding and blood slowing could cause blood to reroute to the opposite side making velocities in the right IJV much higher and turbulent – resulting in pulsatile tinnitus. The smaller diameter in the upper half that you mentioned could also be adding to the turbulence.
I did get a an evaluation for TMJ - no issues found there.
Thanks again for your analysis - very helpful!
Thanks for your reply. I did not know about “military neck”. Will definitely look at the exercises you mentioned.
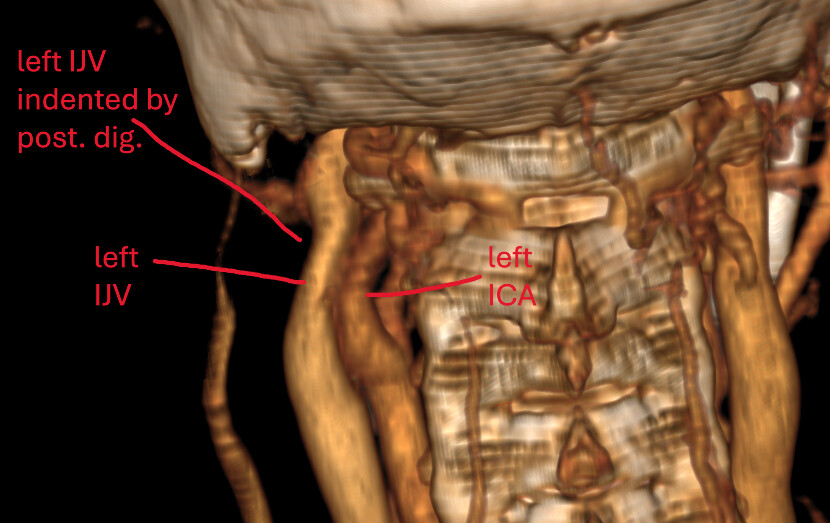
@chrEagle those are logical explanations I think! The compression by your digastric looks worse on the left (seen in image #3). Where I have labelled your left ICA and left IJV, the IJV is pancaked between the left ICA and the posterior digastric. The posterior digastric touches the right IJV as well, but compression is not as bad. I think it moreso has to do with your left ICA pushing your left IJV into the digastric. Because on the right side you don’t see compression by digastric, but you also don’t see compression by the ICA. So I think the tortuous left ICA is a pretty significant culprit here.
@TML, I think you are spot on in your analysis and have identified the key problem on this side. It’s a hemodynamic compression issue rather than a neurogenic one.
Do you have the slide number of image 3? I will try and reconstruct in 3D and share it with my doc.
=====================================================================
AI evaluation:
![]() Left Internal Jugular Vein (IJV)
Left Internal Jugular Vein (IJV)
Appearance: The left IJV is significantly compressed, appearing flattened or “pancaked” in cross-section.
Interpretation: Classic extrinsic compression of the IJV between the left ICA and posterior digastric, forming a C1/digastric/ICA corridor. The IJV is trapped in this soft-tissue triangle, not a bony entrapment (i.e., not primarily due to styloid or C1).
@TML, would this still be considered Vascular Eagles?
Thanks!
@chrEagle I don’t have the number, and it may be hard to see in 3D. Most radiologists use the axial view (the view I posted) when assessing for compression anyway, so it may be better to just show your doctor image #3 and explain to them that you think your left ICA is compressing your left IJV (and against your posterior digastric). A surgeon can move the ICA which may be all you need IJV-wise. However, you do have those small pockets of calcified stylohyoid ligaments and I wonder if they are contributing to any symptoms. Doesn’t appear they are contributing to anything vascular-wise at least.
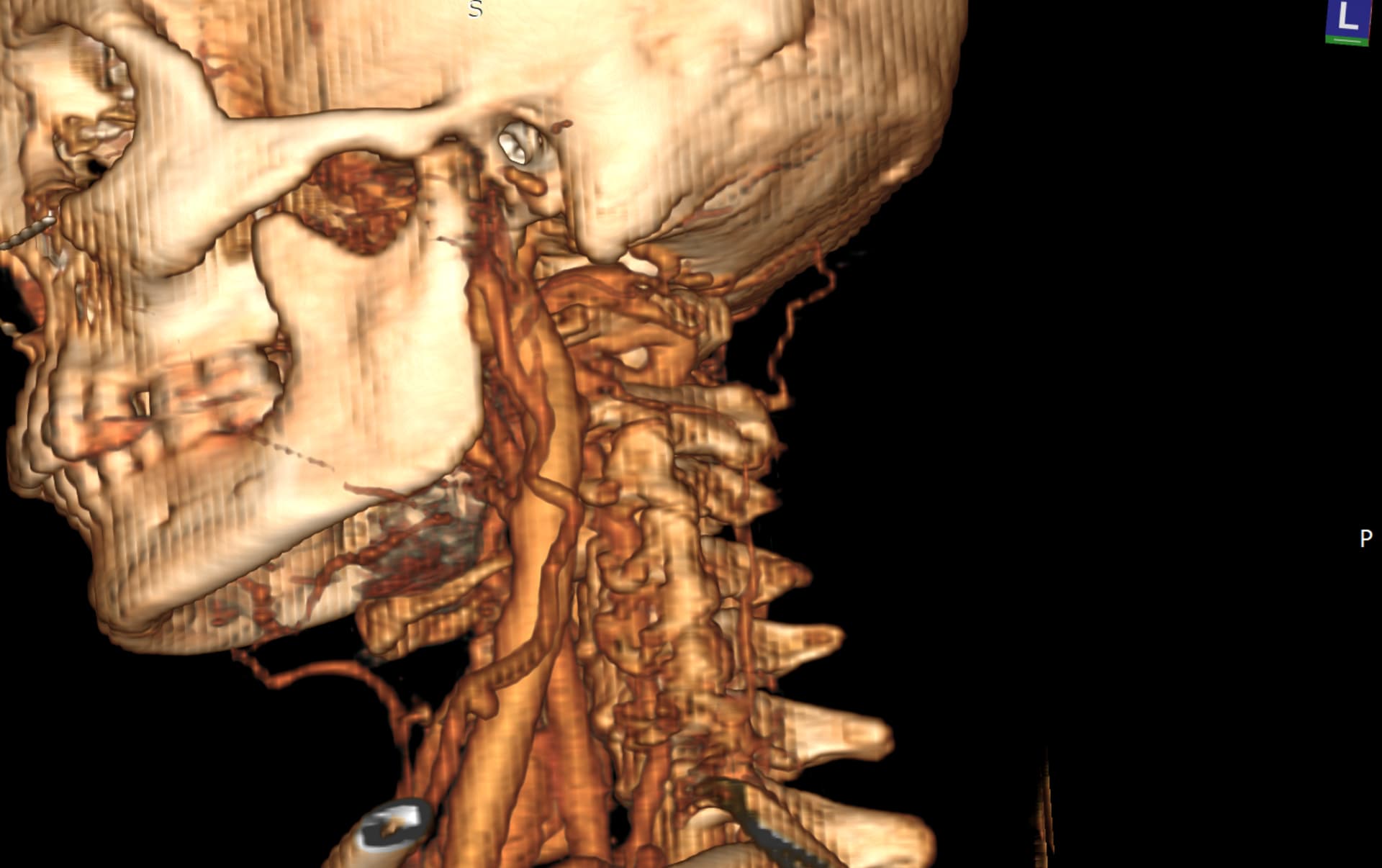
You can actually see the tortuous left ICA run into the left IJV in the 3D model I posted:
@chrEagle I re-downloaded your CT to get better 3D images of the compression in question.
See attached. Hope this helps!
@TML, Thank you so much. This definitely helps!