Hello Everyone,
Greetings from the large island of Australia.
Right styloid process measures 4.6cm in length and left styloid process measures 4.4cm in length - “Mildly elongated styloid processes”






Perhaps my story might start In 2020 after a car crash, I would describe my symptoms at that time as severe whiplash, very sensitive neck and upper limb pain that never went away. If anything more symptoms appearing over time. Intermittent weeks and months of debilitation, originally thought to be something like CFS / Major Burnout.
Life is hard, no practitioner truly listens, people don’t understand. Luckily or tormentingly I am extremely stubborn and try to compensate as best I can, in between the occasional rotting/giving up periods.
My symptoms Include:
- Being unable to look down, without rapidly worsening symptoms or it gets to that point anyway.
- Vision issues - Blurry / double vision - it’s intermittent and variable in nature, I believe head position also influences it. Optometrist cant get my glasses right with the addition of prism and slight magnification, but I can read/test at 2020. Sometimes my vision wonders and I cant focus on anything.
- I also experience this strange eye leaking (usually 1 eye - outer corner), which only happens after I lay partially reclined with my head back and turned after 10-15 mins, that happens when I have a dull headache, or after activity, often when i first wake up. This leaking is associated with a profound feeling of relief and brain fog elevating.
- Hearing - I would describe as muffled/compressed, It makes music often un-enjoyable and i have difficulty understanding people sometimes. It also feels “full” - again i can somewhat reverse this with head position
- Occasionally ill turn my head or look down with loud sudden tinnitus in one ear, again reveled by head position.
- Often have some ringing/tinnitus that gets louder the worse i am, also pulsate tinnitus sometimes as well, often accompanied by a horrific headache.
- Dizziness
- Vertigo
- Head and eye pressure
- Positional sinus/ airway issues
- Smell and taste
- Weird nerve pain behind my ear (all round) - also temple
- Jaw pain, teeth pain, scalp, neck
- So overall symptoms like Occipital and Trigeminal neuralgia
- Getting stuck in bed unable to wake/get up
- Hyperadrenergic POTS - positional like symptoms
- Sudden extreme nasua
- Progressive difficulty swallowing - seems to correlate with how symptomatic I am, gets to the point where either it becomes to painful or I cant innovate a swallow, sometimes food gets suck for 10-15 mins (positional relief seems to help here). Smaller things seem to get stuck in throat without impacting/preventing swallow, I feel it release and go down, I think i also sometimes experience this but slightly different where its just the sensation.
- I “choke” if i move my head to far back/ in the wrong position
- I had a barium swallow test - which was “normal” - I would note that my Pyriform sinus stay filled between swallows, and I cant do a full big swallow in one go.
- Talking seems to be a factor in making it worse
- I have a “pointy bony protrusion” in the back of my throat near tonsil that pokes inward (can feel it with my finger) - ENT MISSED THIS! - I wonder if this is what others have described in the forum as the styloid shelf
- Food and drink also goes up my nose quite regularly
- Fatigue
- Headaches / migraines
- I have had these for weeks/ months at a time almost daily at points
- Something seems to trigger Extreme anxiety / panic too, ill be feeling very unwell at the time usually, again usually reversed by position
- Cognitive issues
- Memory
- Speech
- Unable to access things i know i know
- Thoracic / upper back and pain in both arms and hands
- CRPS diagnosis for left hand/arm
- Right hand is newer
- Pain can be on any of the nerve distributions or move around
- Outer 2 fingers on my hands occasionally have blood flow issue - they go blue
- This again I think is positional, I think i have found some positions to reverse it, and triggered by say working at a desk
- Arms above head, (I like to hold my head back and turned) - Both arms will tingle and then go completely numb - unable to move said arm
I have whinged to at least 10 GP’s, multiple physios and a few specialists (Neurologist (really really pissed me off and suggested FND), Sports doctor and ENT), all who all wouldn’t really listen, wouldn’t discuss the logical fallacies of their arguments, and said there was (sort of) nothing wrong with me.
I managed to get a 3D CT after finding the bony protrusion and presenting to a new GP with the dysphagia symptoms. The GP was willing to refer for CT with contrast/angiogram, however its very expensive and not covered by medicare unless a specialist refers it (frustrating).
- The GP referred me to (with my input) Dr Ben Dixon at St Vincent’s hospital - they took a month to send me a letter so say no appointment time, waiting list.
- Also referred me to Dr Michael Elliot (who seems to be the expert in the country) interstate in the hopes he might review over a phone appointment. They contacted me and said he reviewed it and I dont need to see him and I could see Dr Ben Dixon…
- A 3rd referral to an OMFS - who have not gotten back to me and im questioning if that’s the best doctor to see anyway.
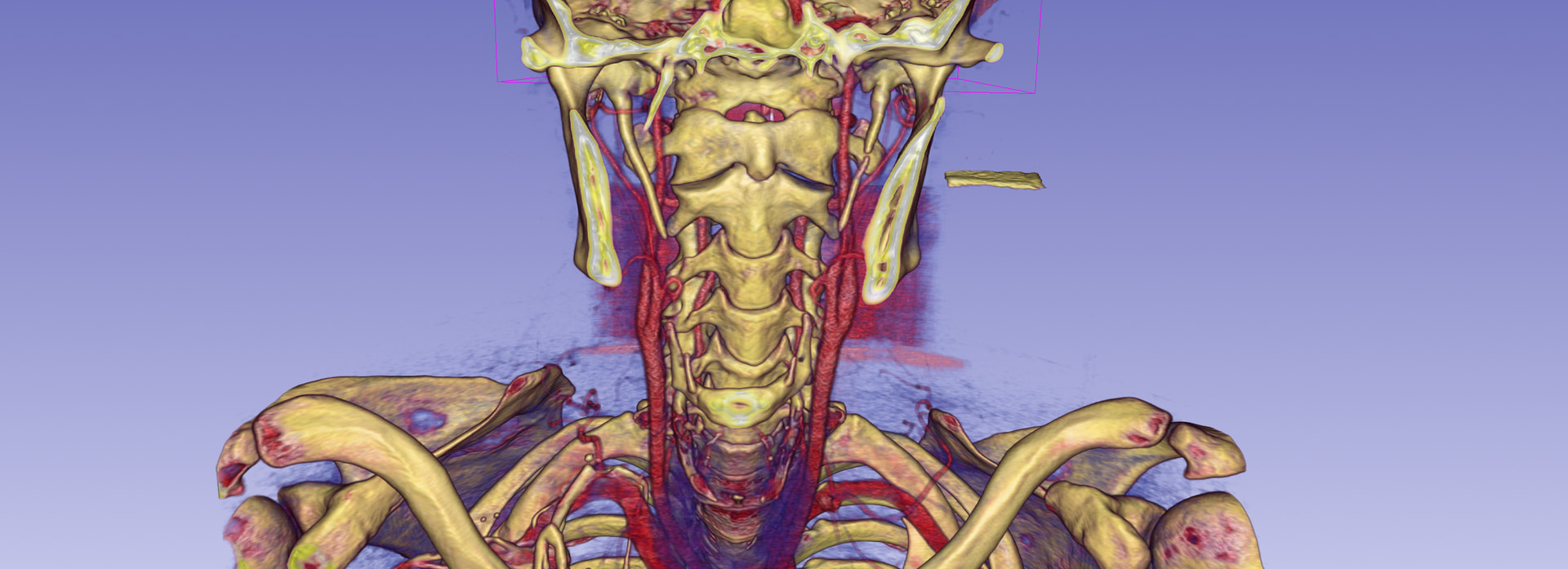
I rendered my CT scan, so ill provide a few images of that. Sure looks like there’s not enough room for the internal jugular/carotid. You’d think that’s enough for it to get taken seriously!
- Also of note, is this what appears to be calcification between dens / C1??
- I had an MRI that I am also pretty suspect on - I don’t believe the Nurologist personally reviewed it. (Anyone on here good at interpreting?)
Recently i also seen an Orthopedic surgeon, for an independent medical review, he actually listened and asked appropriate questions and tests (I didn’t get to/have time cover eagle syndrome type things). He seemed to think I had Thoracic Outlet Syndrome, but I am wondering if/ how much of that might be created by the Accessory cranial nerve?
Overall I am extremely frustrated at the medical system, Its very hard to convey the what and how I am so unwell and doctors don’t seem concerned as it doesn’t follow a particular pathology in 1 area or whatever. I often cant even communicate properly, but its dismissed as anxiety.
I probably forgot a few symptoms… (to many to remember)
Apologies if this is not formatted the best, using a computer/phone to type kinda sucks, and I am (probably) some form of dyslexic.