I’ve been diagnosed with jugular vein compression. I had a telehealth appointment with Dr Constantino and he told me my left side was 90% compressed by my styloid and C1. He told me this was my non-dominant vein. It’s very small on imaging. And with this, I also have stenosis of transverse and sigmoid sinus on that same left side. Constantino told me that my right side was dominant and was also compressed 50%. Constantino told me the right side is where we would have surgery. It was all dependent on catheter venogram and balloon occlusion study. At this time, Constantino was only diagnosing just by looking at my CTA and CTV.
Here’s where it gets interesting. Meanwhile, I went to a local physician and got the catheter venogram. This doctor is well-versed in this area and told me that we needed to look at the left side not the right. He thought the right had enough flow. When he measured my pressures, he told me my pressures were extremely high. Some were 10, 20, 25 and 50. He said also that the pressures were normal on the right and dominant side, despite being compressed 50% by C1/styloid. He verbally told me I had stenosis on the right side (large/dominant side) of transverse and sigmoid sinus- calling at tandem stenosis. Can that be? Is it possible to have a narrow transverse sinus in a very large dominant jugular? Verbally said my vein of Galen was small.
I’m extremely symptomatic. These are all the typical symptoms that we all have here: brain fog, dizziness, pain in the back of my neck, extreme and severe head pressure, unable to sit or stand longer than 15 minutes, severe headaches, nausea, feeling like I’m falling. Homebound and in bed much of the day. Symptoms are pretty severe.
I had not got my official catheter venogram report yet by the time I had my next appointment with Dr Constantino. But I verbally gave him my pressure numbers. He was shocked. He said I was definitely a candidate for surgery. However, I didn’t tell him which side had the pressures. It was from my non-dominant small side. So there might have been some confusion there. I emailed the office, letting them know that these pressures were not from the side that he wants to operate on! Constantino told me that they always operate on the dominant side
My concern here is that I do not want a surgery when there is no pressure on that side. I don’t think it would work! The surgeons hardly ever work on the small side. Also in my catheter venogram report, the NIR said that my dominant side was my small side. Not the large side. Has anyone heard of that? I’m just confused all the way around.
Since Constantino had not looked at the venogram report, he was going off images only.
I’m wondering if any of you can help here to see what the normal protocol is for surgery. I’m afraid of going in and having it not work because the NIR said pressures were fine on the side that Constantino wants to work on. It makes sense to do the side that is small, but I know they don’t do that because it may not get enough blood flow. I feel Constantino had his mind made up based on images and his protocol on how he does his surgery.
Any comments are greatly appreciated!
@Luckee7 Similarly, I had a more fully stenosed non-dominant IJV and partially stenosed dominant IJV. Dr. Nakaji suggested starting with the non-dominant side in hopes that opening that up plus the partial flow on the other would be enough to not need a second surgery. Once in surgery he was able to see that the veins on the non-dominant side were likely too diminutive to support good flow. Still we waiting about 6 weeks to see what happened with my symptoms. Ultimately I needed the dominant side done which in turn eliminated most of my symptoms.
Thank you for your response. That helps me immensely. Can I ask what all Nakaji did? Were your pressures high also? Did you have pressures on the dominant side? Glad you’re feeling good now!
I’m sorry I meant to reply yesterday but got distracted!
Normally we’ve suggested that getting the dominant side first would seem to make more of a difference to the flow in that vein & help your symptoms resolve quicker; if you don’t have much flow in your smaller side, everything goes through the dominant side, so if that’s also compressed as you say to 50% then I would’ve thought to remove that first would have more impact?
But reading through an old discussion, @anon67578920 posted this:
‘As Doctors Peter Nakaji and Michael Lawton wrote and as I think based on hydrodynamics, it is necessary to remove compression from the non-dominant side. Why ? Because the resistance of the weak side (non-dominant side) is greater, and when you release the dominant side, the blood flow will increase, but on the non-dominant side it will decrease (because fluid, like electric current, flows more along the branch where the resistance is less) and in the end you further reduce blood flow on the non-dominant side. As a result, you get headaches in that hemisphere, etc. In general, I think that if there is significant compression on both sides, then you need to operate on both sides after some time. Why ? Because after 1-2 years, the distribution of blood flow will improve and the veins will begin to change their sizes and in the end, on the one hand there will be a small deficiency. Of course, there won’t be any special or strong symptoms, but still. only if you have poor metabolism and are prone to arteriosclerosis, the transverse sinus may gradually, over a couple of years, thrombose due to low speeds.’
So there you go, not any clearer? Here’s a link to the discussion: 1 year (almost) post right sided styloidectomy/C1 resection update - Symptoms and Treatments - Living with Eagle
I’ve not heard of anyone being told that their dominant side was the smaller side before either!
I’m afraid I don’t know anything about transverse and sigmoid sinus stenosis, so can’t comment about that…
We do suggest that members try & get at least 2 appointments for opinions, but we have seen some members who have seen the more well known VES get differing opinions, which then makes it extremely hard to decide what to do! I guess sometimes you have to consider your gut feeling & how confident you feel with the doctor, and ease of travel etc for the surgery… Is it worth trying to get a consultation with Dr Nakaji in AZ? Although he does requite a CT venogram pressure manometry I believe- some members have travelled to get that done with Dr Mehta and then been assessed for surgery within a few days. But that seems to vary too!
Thanks so much for your reply. This makes sense. I may send images into Nakaji to get his opinion. Not sure if he would take a catheter venogram From someone other than his person though.
You’ve given me information to further research. Thank you so much!
I clarified with the NIR that my dominant side is indeed my large side. The NIR said there are other, what they call “dominant sides” for other parts of the Venous system. I didn’t want to steer anyone wrong on here!
Just FYI—Dr Nakaji accepted a catheter angio/venogram from someone else in my case. That was just a couple of months back, so it seems probable.
@Jules Fascinating quotes from Nakaji and Lawton about which side first. It is not consistent with what Nakaji (or Hui) recommended for me, but it is a very interesting subject, I think, and this is a somewhat unusual take.
He ultimately declined to do my decompression because of comorditities. And in fact based his initial offer on the venogram alone–no consult or medical history. I was really disappointed, but I suppose we end up where we need to be, particularly if we do all we can to make that happen. I have now had a styloidectomy with another surgeon. Just a week post-op but so far so good.
Thank you for your response Yes, we all end up where we need to be. Nakaji seems to be very selective. We will see what happens with mine. Glad you are doing well post styloidectomy!
I have also found a doctor in Southern California that wants to do a C1 shave only on my non-dominant, small side, with the extremely high pressures. (90% compressed with min drain). Again, they said my right, dominant and open side, even though compressed 50%, had no pressure or very low. (this is a completely opposite approach that Constantino took.) The NS said my I JV is “draped” over the transverse process and not in contact with the styloid. The NS does not do styloid removal.
I am tempted to go this route for a few reasons: ease of Travel, less invasive procedure, ease of scheduling. This doctor has not done many of these procedures like the others, albeit the ones he has performed have been successful. I do know that styloid removal remains part of the standard procedure in the surgery, and there’s got to be a reason for that, but I am also dealing with cervical instability and researching surgery for that as well. I am not wanting to disrupt that, especially with the surgery Constantino wants to perform.
I am a case with extremely severe symptoms. Due to the high-pressure’s.(NIR confirmed pressure is in the 50s while upright) I am unable to be upright for longer than about 15 minutes, unable to work, homebound, and for the most part bedbound. Also have stenosis in the transverse and sigmoid sinus on both sides. Greater stenosis on the side with the non-dominant side.
I have sent images to Nakaji as well and with that there is NS confidence, more experience, ease of Travel and scheduling.
The SoCal NS and NIR are both confident that this would take care of my issue. But the approach with the small vein first is not taken on with many of the NS’s.
I know many of you have gone through this process, therefore having great knowledge. Your thoughts?
@Luckee7 I had my IR venogram done by Dr. Amons at UCSF. I had elevated pressures on both sides. On the left side(non-dominant side) Dr. Nakaji did a styloidectomy and C1 shave. On the right side he was not able to reduce C1 due to some anatomical variants but he was able to reduce the styloid enough to allow the IJV to be free of C1. That side was also greatly compressed by several muscles and the carotid sheath which he was able to release.
I’m not sure that a C1 shave is any less invasive or any easier a surgery to have, it’s in the same area as the styloids so I would think carries just the same risk, if that makes any difference to your thinking, but that’s just my opinion, your doctor may disagree and would know more!
Do you have any nerve pain etc, other ES symptoms along with the vascular symptoms? If you do then having the styloid removed as well may help…
I appreciate it’s a difficult decision with the surgery, especially as you’re so debilitated by this, and hopefully others’ can give you their experiences, but I guess ultimately the best advice is to get another opinion, perhaps from Dr Nakaji if you can, and to make your decision being guided by one of the doctors you’ve seen, whoever you feel most confident in…we’ve had other members who have seen several of the best known VES doctors and been told different things, it’s so hard, sending you a hug
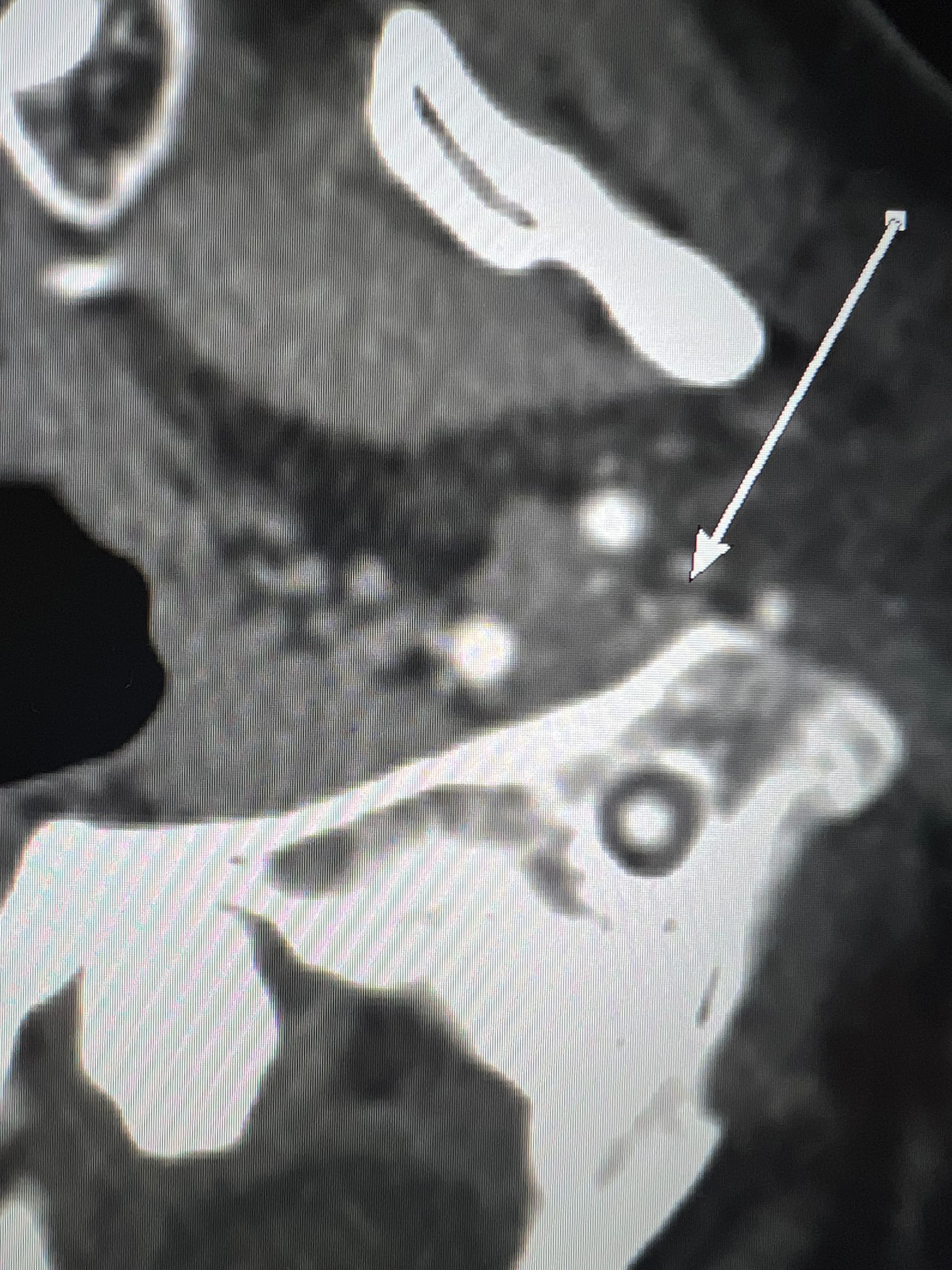
@Luckee7 - I’ve marked some vascular structures that are above & beneath your C1 vertebra that I haven’t seen before in other imaging so am not sure what they are or if they could be involved in causing symptoms. Those above C1 appear to be “sitting” on it which appears to be causing some minor compression of those sections. They could be collateral veins, & if so, then they’re likely contributing to skull base/occipital pain.