Still, there are symptoms associated with nerves, compression of the atlas region, innervation - the vagus nerve, ganglia and accessory nerve. That’s why the symptoms are so rich and different from person to person.
In any case, relaxation of the neck muscles and exercise will give a partial positive effect, inflammation - muscle volume / hypertrophy will decrease and there will be more space for nerves and blood vessels.
1 Like
Anything that can be done to help reduce inflammation does help reduce symptoms. Thank you for making a good point.
Guys, there is a complex here, part of it is a displacement of the atlas forward in relation to the skull, for those who have a dislocation of the atlas (but in this case, compression of only one IJV) - this is the tip of the iceberg, i.e. part (perhaps a strong forward displacement will play a major role) and in addition (often as the main cause) it is the stylohyoid process or the large transverse processes of the atlas. Possible muscle adhesion, adhesion/fusion of the stylohyoid muscle and digastric muscle.Which causes both compression of the IJV and innervation of the nerves. as well as a slight narrowing of the spinal cord

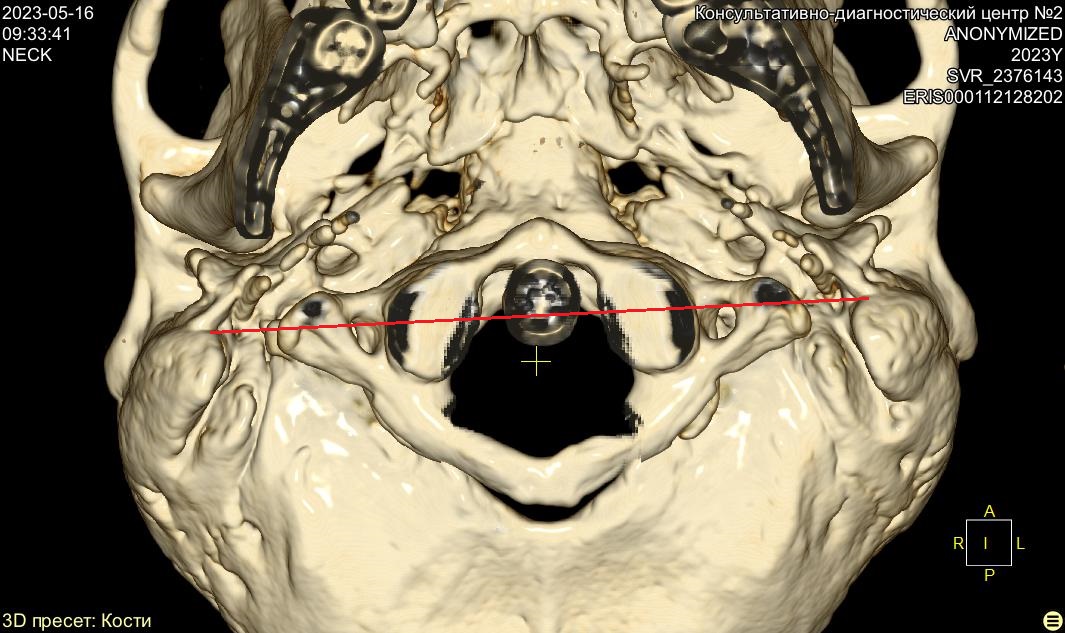
This is a comparison of my picture and the picture of another person Yaroslav with eagle syndrome, as you can see, his atlas is shifted forward more than mine (do not confuse it with a dislocation), but I have larger transverse processes of the C1 atlas.
Therefore, I think that sleeping on the stomach, face down on a couch with a hole for the face (so that the head is slightly lower than the thoracic region, the correct lordosis and angle) and relaxing the neck muscles, including the muscles of the craniovertebral junction, will shift the atlas a little back and for the majority there will be a positive effect, partial or more.
1 Like
So in principle it’s the same if you turn the body into supine position with the head elevated on an orthopedic pillow?
See my old post with this speculative question about what happens if you sleep with your head slightly elevated to reduce gravity effects and “open up” various spaces in the neck
1 Like
I guess, yes . But the height of the pillow needs to be adjusted. An orthopedic pillow of a certain height, and I did that, I put a towel under the pillow so that it was higher, and it’s a little easier to sleep on your back that way too. But the atlas C1 in this case will not move back, because there is no relaxation and a certain directional stretch of the neck. (i.e. the head is lower and the cervical vertebra is slightly higher)
2 Likes
There are modular pillows with some removable parts, also some pillows made of small cubes of memory foam that can be tailored to individual needs. Worth trying. I found it quite comfortable when using the one that can be stuffed as much as you need to achieve height/stiffness/shape.
Another option people discuss is inversion tables to reduce gravitational load (and effects) on the whole spine, though some like it some not. Obviously it’s not suitable for sleeping due to impact on blood flow, but merely for short relaxation.

1 Like
I’ve often thought of trying an inversion table for my spinal issues but I can’t keep my head down like that for long w/o getting a headache. It does look super comfy to me though - letting gravity do the work of opening up the spine!
TOS and compressions and trombosis mechanical damage /dissection brachiocephalic vein (valve ) and artery ,and embouchure, entrance, beginning vertebral arteries
https://istina.msu.ru/publications/article/25094379/
Coexistence of arterial compression in patients with neurogenic thoracic outlet syndrome - PubMed (здесь несколько)
Owen P Palmer 1, Fred A Weaver 2
Thoracic outlet syndrome in a patient with absent scalenus anterior muscle - PubMed (аномалия отсутствие одной лестничной мышцы и наличие симптомов nTOS, вот почему ребро, а еще лучше остиосинтез 1го ребра и ключицы )
Regrown first rib in patients with recurrent thoracic outlet syndrome - PubMed (рецедивы и повторный рост 1-го ребра, вот поэтому лучше остиосинтез еще тем более если оно способно на такой рост)
Вот РЕДКИЙ СЛУЧАЙ компрессии к примеру плечеголовой вены между дугой аорты и грудиной (ключицей)- нарушение церебральный кровоток
Atypical thoracic outlet syndrome and reverse flow thromboembolism - PubMed (два пациента с церебрал недостаточностью)
Migraine complicated by brachial plexopathy as displayed by MRI and MRA: aberrant subclavian artery and cervical ribs - PubMed (один случай мигрени )
Scheuermann's disease as a model displaying the mechanism of venous obstruction in thoracic outlet syndrome and migraine patients: MRI and MRA - PubMed (мигрень и т.п.)
Neck and brain transitory vascular compression causing neurological complications. Results of surgical treatment on 1,300 patients - PubMed (цитата сноска не понятно но про ишемию мозжечка и т. п.) New concept regarding chest pain due to hypoxia of the internal mammary arteries in more than 1,600 operated patients with cerebral thoracic neurovascular syndrome (CTNVS) - PubMed
(цитата ) https://www.minervamedica.it/en/journals/panminerva-medica/article.php?cod=R41Y2002N01A0047
A woman post scalenectomy and first-rib resection with dilated vertebral venous plexus and a facial rash - PubMed еще интересная
такое отступление https://www.apicareonline.com/index.php/APIC/article/download/1230/2037?inline=1
добавил еще статьи
A woman post scalenectomy and first-rib resection with dilated vertebral venous plexus and a facial rash - PubMed A Woman Post Scalenectomy and First-Rib Resection With Dilated Vertebral Venous Plexus and a Facial Rash.pdf - Google Drive (Женщина после травмы в бейсболе инсульт левой ВСА ,сложный случай с венозным сжатием и затрудненный венозный отток, и про позвоночное сплетение вен очень интересная статья. Здесь связь TOS с венозным оттком , как я предпологал что возможно и сжимает позвоночные вены Redirecting)
001 важно.pdf - Google Drive
Maybe when I slept on my stomach, the muscles of the neck relaxed, including the scalenus muscles, and thus the hypertrophy decreased, the volume of the scalenus muscles decreased, this reduced the compression of the vertebral arteries. Maybe the scalenus muscles and atlas, i.e. in complex. I am now recalculating the volumetric blood flow through the vertebral arteries, using ultrasound images.
1 Like
I counted manually from the images. Based on the average maximum speed TamMax, I got 77 ml/min on the right, and 80 ml/min on the left, of course (Normally, in a healthy person- 83 ml/min + - 35 ml/min, one artery ,depending on the structure of the vessels and brain volume. According to MRI values, MRI is better than ultrasound, but with my methods, using ultrasound, you can get accurate values with an error of 5 to 10%, which is quite accurate). But preliminary, according to the correct speeds, the averaged time speeds of TAMV, it will be approximately with a reduction factor (closer to the gold standard) 60-65 ml/min per vertebral artery, and this is already a rather low blood flow (volumetric blood flow). But as I wrote on the basis of hydrodynamics due to compression IJV, may be less total blood flow (VA+ICA) / I still need to calculate ICA
These are interesting observations.
I tend to think that blood flow is so variable during the cycle of motion and course of the day that it’s practically impossible to accurately measure the “universal” numbers, and I actually yet to see any study that shows the same person’s volumetric flows during different activities, at different times of the day (when the blood pressure might be very different), and during various conditions, causing possible inflammation and additional compression in the neck.
I’d suspect it’s possible to come up with some numbers +/-50%, but again that’s very speculative as I really don’t know about how much blood is needed for the brain to stay just awake, do menial task, do mentally intensive task, or be under stress.
I would guess, it would be more useful/meaningful to measure O2 and nutrients reaching the brain. As far as I know (though I might not know ![]() ), the brain doesn’t have extensive nutrients/O2 storage capacity, thus depends on the constant blood flow delivering sufficient amounts of O2/nutrients.
), the brain doesn’t have extensive nutrients/O2 storage capacity, thus depends on the constant blood flow delivering sufficient amounts of O2/nutrients.
if you conduct an examination and measurements in the same state, i.e. at rest, the difference between these examinations will be no more than 5-10%, since your pulse and pressure will not vary much (be different). But if you do an examination after physical activity and your pulse is 80-90 beats per minute and your blood pressure is 140/100, then of course there will be a strong increase in volumetric blood flow and if you compare the examination at rest, there will be a big difference. But all examinations are carried out at rest (without physical activity, the number of heart beats/pulse and pressure are approximately the same, a small difference does not introduce a large error) and there will not be a large difference of about 5-10%. a few specialists even measure pressure and pulse, but this does not make a big difference/error, if you are at rest, calm - your pulse and pressure will be approximately the same (if you have a healthy heart and there are no problems with the pulse / tachycardia, etc.) d.). In a healthy person, the pulse during the day, during normal activity and in a calm state, is approximately the same. A change in pulse by 3-5 beats or pressure by 10mm will not introduce a significant error/change.
research links above. And as an addition, there is also a concept in hydrodynamics: the flow-pressure characteristic of the pump and hydraulic system (pipeline system). The heart is the same pump, and the pulse is the amount of rotation speed/RPM/min of the pump. and if you look at the characteristics of the pumps, a small change in rotation speed/rpm does not significantly affect the flow rate (volume of liquid pumped)
Of course, it is more accurate to measure pulse and blood pressure. but it’s a small difference
oxygen consumption O2 also increases with physical activity, mental activity, etc. The need for oxygen provokes an increase in heart rate, i.e. they are directly proportional. What buffer for blood?)))) The calculation is carried out in cycles. You don’t have a 100-liter tank in your head to hold liters of blood there.
It’s hard for you to understand, I understand that. But in addition to volumetric blood flow, the problem can be determined by the ratio of volumetric blood flow (which was measured at almost the same time). Va/ICA *100%= %
Well, the spleen is holding some amount of blood that can be quite quickly put into the circulatory system under certain circumstances to avoid shock; muscle cells store glycogen, which can be released and converted into energy; meanwhile brain is sort of isolated system totally dependent (perhaps, not 100% of that) on the constant supply of blood and starting to malfunction and then die rather quickly if the blood supply (oxygen and nutrients, actually) is cut off.
I am thinking (while obviously ignoring your attack on my personality vs my thoughts and process of thinking, perhaps indicating your lack of acceptance of different opinion and believing that there is only one Truth, The Truth, and only someone higher in the food chain is entitled to question about it), could it be that our internal organs are sort of well adapted to be deprived of oxygen/nutrients and survive for quite a long time (think of the accidents when people lose their hand/arm which is reattached only a few hours later and eventually comes back to life), except the brain? It would be interesting to learn more about how the cells store “the fuel” and why brain cells are so ineffective from this perspective, esp.from the evolutionary perspective.
Another thing is vasoconstriction effect, which obviously affects the volume of the circulatory system. It would be interesting to know where that blood ends up in the meantime until the volume of the arterial system recovers. I’d guess there is a possibility that it remains in the veins thus increasing venous pressure, but I’m not certain of this. The other day I was looking for any research on this but couldn’t quickly find anything significant.
2 Likes