Hi all, I have opted for surgery after years and years of symptoms in the hope this is the root cause and I can start to feel like myself again. I’ve not had an official diagnosis of eagles because they don’t seem to know much about it here in Scotland. But my ENT consultant has said my elongated styloid process is the cause of a few of my symptoms and not all, even although on here you all seem to have the same symptoms I have had over the years.
I have decided on the intra oral TORS approach for left styloidectomy. Has anyone had this and had positive outcomes from their symptoms. My symptoms vary each flare, but mostly I have brain fog, sever fatigue due to living in the dark with these symptoms, fullness in left ear, muscle pain and tightness in left side of head left base of skull left shoulder and trapezius. Pressure in left side of head eye and face. Light and sound sensitivity, tinnitus that comes and goes like a power drill and vibrations in my head at times. Globus sensation comes and goes and can feel the styloid getting stuck in my throat if I look to the left yawn or cough. I also get lightheaded like I can’t focus but have never passed out. I have also had a left sided haemeplegic migraine where I had left sided weakness all down my left side. I have also had bells palsy left side, I’m not sure if this is linked or not. I could go on but these are the main ones that are mainly there most of the time.
Any tips for surgery or success stories would be much appreciated.
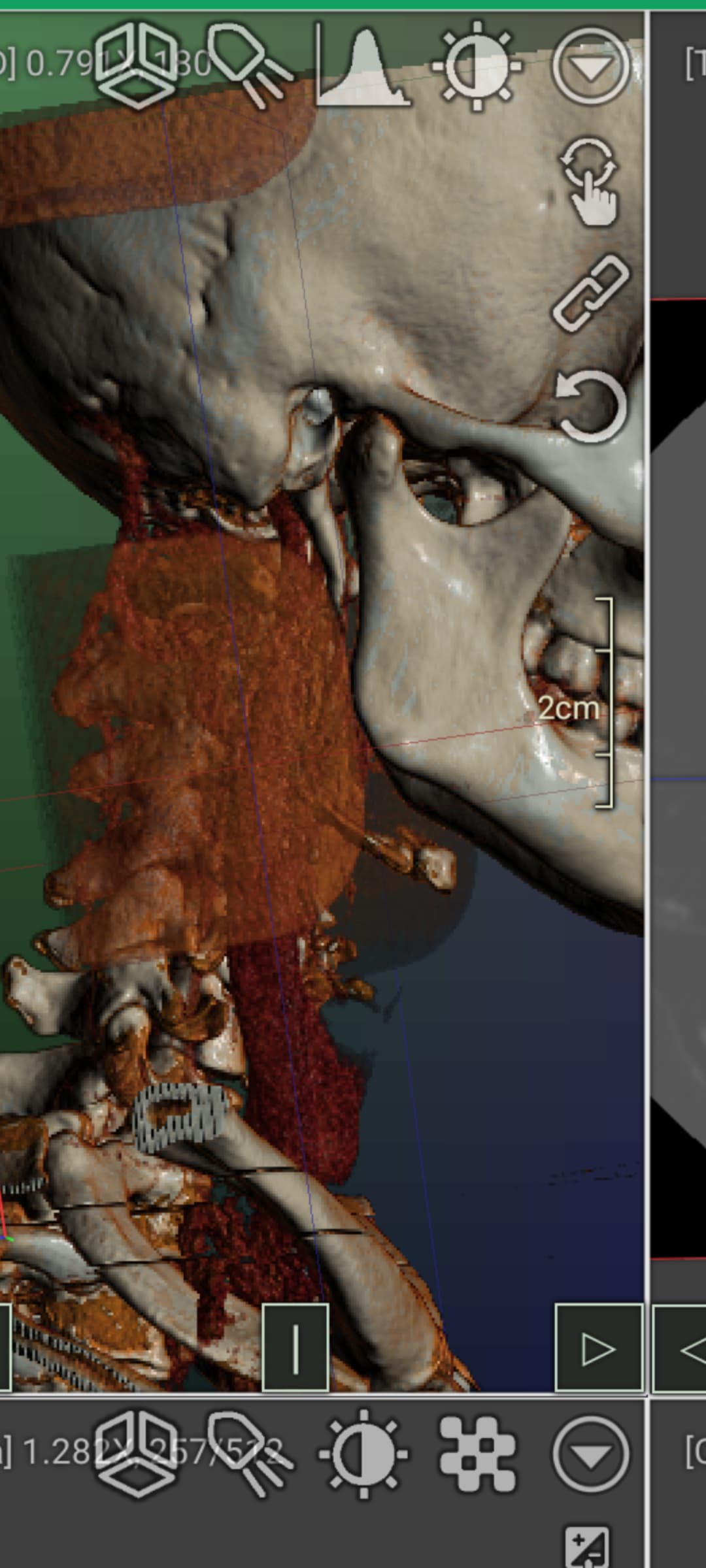
Wow @Max330 that is a gnarly left styloid. Thick and long. No wonder you have been living in agony!
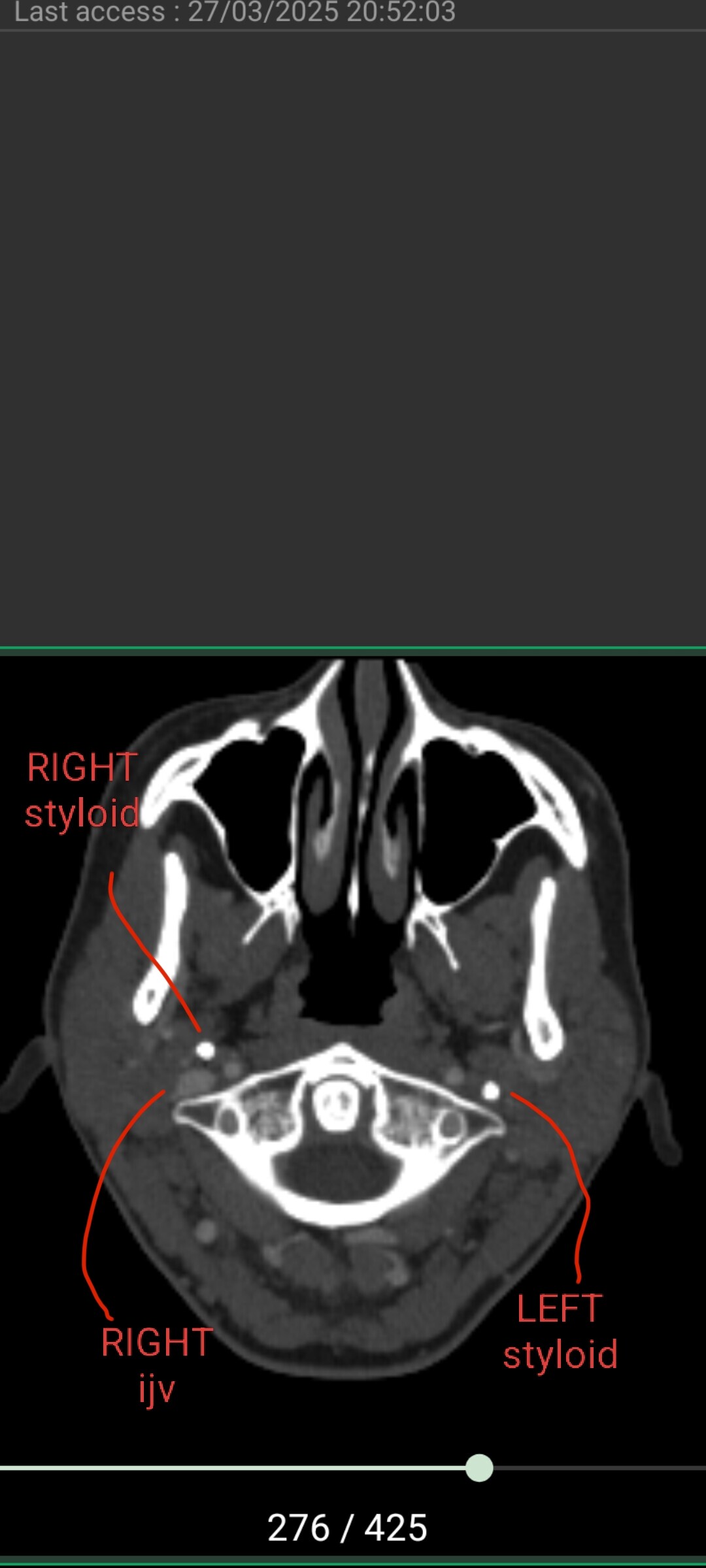
Can you go to the axial view of your original CT imaging and go to the area of C1? I’ve uploaded my own imaging to help you find it. I’ll help you locate your IJVs to see if they are getting compressed. I suspect they are based on your symptoms.
I’ll let others comment about the intraoral approach, as I’ve not had a styloidectomy at all (yet!).
@Max330 , actually there is one thing I want to mention about intra oral surgery (based on what I’ve learned via this forum). Often in intra oral the surgeon just trims the styloid, rather than cut it down to the skull base. This is adequate for some members, but is not adequate for those who are experiencing IJV compression between C1 and styloid. The surgeon can’t access as high up on the styloid via intra oral approach. This is why external approach is often preferred. But we shall take a look at your IJV to see if that is a factor for you (I’m not a radiologist fyi, just sharing my knowledge)
@Max330 - We have a couple of members who’ve had TORS intraoral surgery & have had good outcomes, but as @TML said, it all depends on how close to the skull base the styloid is cut. I believe w/ the TORS surgery getting close to the skull base is more possible, but it would be good for you to ask your surgeon how short he intends to cut your styloid before your surgery.
Your symptoms sound to me more like your carotid artery is being affected since you’ve had some stroke-like symptoms which usually come from carotid irritation or compression. It can also cause brain fog, eye pressure, & facial paralysis type symptoms. Most of your other symptoms sound nerve related, & w/ a styloid as massive as yours, there are likely numerous nerves that are irritated. I think getting that nasty thing out of your neck should produce good results for you if your surgeon cuts the styloid short enough.
Here’s a post from the first person on our forum to report a TORS surgery. Note it’s from 2021: adriene61
I didn’t have the throat or tongue pain. I had wild headaches, positional, electrical, stabbing. Face neuralgia. Shoulder and neck pain. Double and blurry vision. I had bilateral intr oral syloid and process removal with the Davinici robot Nov 2019. I was 80 percent better immediately. However I have many other health issues. Nothing to do with Eagles Syndrome. He did take everything out and he warned me of all the risk and that fragments can break off in surgery. Unfortunately I started having temporal pain and jaw pain recently and he did a CT scan and I had part of my process break off on each side and calcify, entagled in nerves. He was going to take both fragments out Feb 26th but he got in there and he said he had to move so much around he felt better waiting on the right side until the left recovered. All went great and I am doing the right side next Friday. I can’t say enough about him. One of the best doctors/surgeon you will ever find. Best of Luck to you!
(from this discussion thread - Anyone else have these symptoms.......? - #8 by adriene61)
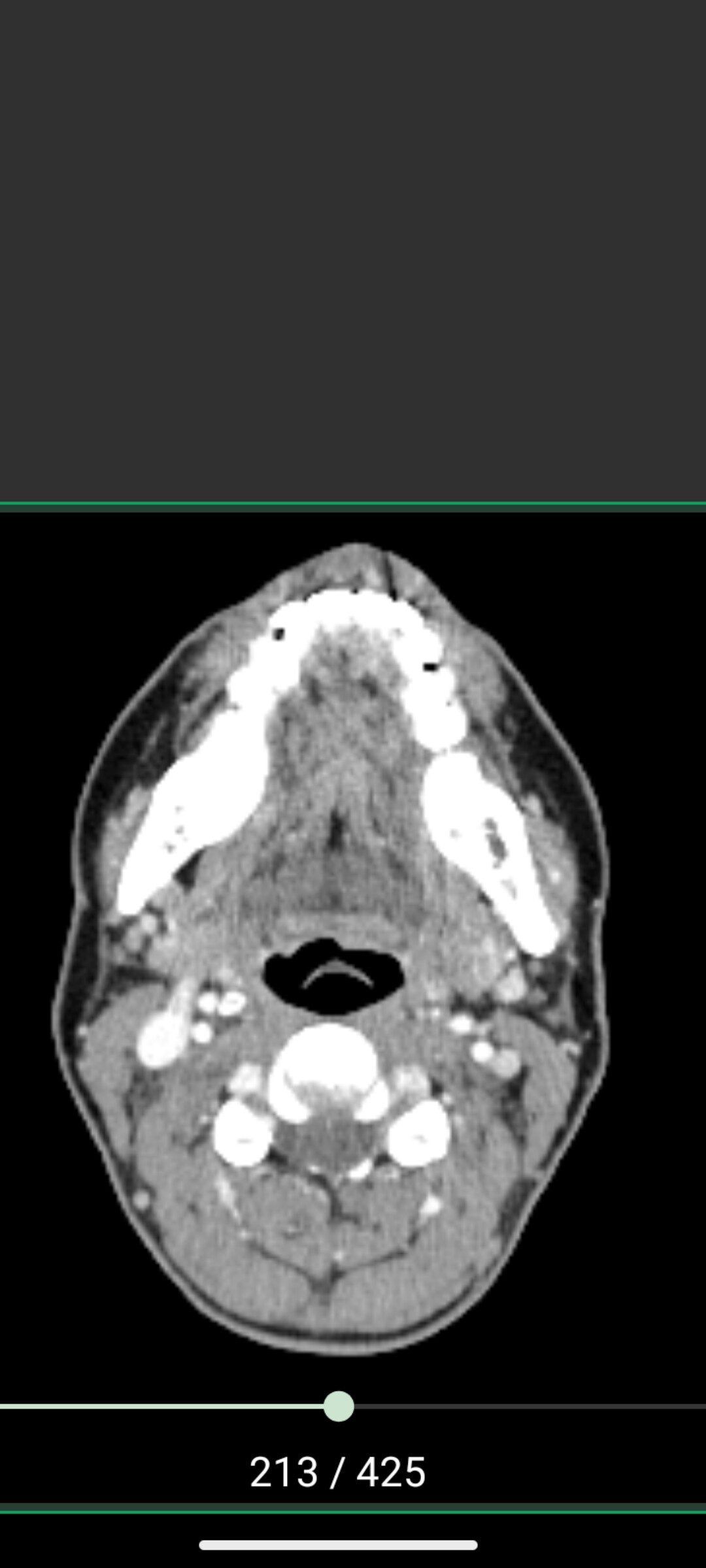
Thanks for your reply, Is this the view your looking for? The surgeon plans to only take as much down as he thinks is safe to maintain stability. As there not really any surgeons in Scotland who do this procedure or know about eagles I need to go with it and hope for the best.
This is my right one which is within normal range but to be still looks like it’s thick and calcified, I’m wondering if they are calcifying due to CCI as my symptoms also link with that and I’ve read that’s why the styloids calcify to give structural support to the neck, I’m worried I’ll lose that if the styloids gone completely.
Have you received imaging for CCI and been diagnosed? If not, symptoms that you think are instability may actually be ES-related such as IJV compression.
I also theorize that ES patients who do have CCI as well have CCI due to muscle imbalances caused by compensating for ES. Besides those who have conditions like Ehlers danlos syndrome or other conditions causing CCI directly. That’s just my theory though. I think once styloids are removed and your able to perform proper, full range neck movements and make use of your deep neck flexors your instability will reduce. We need research on ES and neck muscle imbalances!
@Max330 , the situation in Scotland seems to be getting worse, we’ve had several members who have had real trouble getting anyone to listen… The intra-oral approach isn’t ideal as obviously you know but it doesn’t sound like there’s any choice, and hopefully it will work out and be successful for you. Here’s a link to @Lemontree ‘s discussion, as she had surgery with TORS, idk if it’s the same surgeon:
You could always click on her avatar to send her a private message if you want to chat more…
Regarding the instability, doctors can’t agree on whether the styloids grow to stabilise the neck if you have CCI, or not, & whether removing them will make it worse…We’ve had members whose symptoms improve with surgery & some who feel their neck is more unstable, but when you have a styloid like yours it can’t be good leaving it in!!
Let us know if you get a definite date for surgery!
I just had stylohyoid removed and IJV decompression. For what it is worth, surgeon told me the intraoral approach is not the way to go if you have the symptoms you have particularly, and likely at all, for reasons already covered in terms of getting the whole thing and decompressing the C1. Intraoral has far higher rate of complications. Plus, he noted that if it fails, going back in becomes doubly hard for landmarks and scar tissue. These ligaments are not anchoring your head. My neck and trap move better now than before surgery.
No I’ve not had up right imaging for CCI investigation all my images through the years have been lying flat. Just some of my symptoms seem to match with CCI.
I know it’s not ideal at all I feet like I need more imaging and definite diagnosis but with NHS it’s limited. As Jules says there’s not a lot of options here and my styloid is clearly enlarged and needs to be reduced at least and hope for the best. He did say he could go the external approach but it did seem more risky the way he planned to do it, so I opted for intraoral. I’ll keep you all updated. Thanks for the replies it’s good to know people out there understand.
Pardon my language, but holy crap you might have the tightest space between a styloid and C1 that I’ve ever seen. Your LEFT styloid is so jammed up against your C1 transverse process that there isnt even an IJV to be seen. Probably so squished it doesn’t have contrast in it. Your right IJV is also compressed (not nearly as bad in comparison). IJV compression causes symptoms like pressure headaches, eye pressure, brain fog, memory difficulties, ear fullness, and dizziness (leading to balance issues). Your vagus nerves run between the IJVs and C1, which means they are probably compressed too. Vagus nerve compression can result in acid reflux, digestive issues, fight or flight response and HR and BP issues. I suggest a pillow wedge to sleep if you don’t already have one. Will help the IJVs drain with your head above your heart over night. A styloid-C1 distance in a healthy individual is about 9mm. I’d be surprised if you have half a mm on your left side.
I think with this knowledge you certainly should become 100% sure whether the surgeon plans to cut the styloid above the level of C1. You definitely need it trimmed higher up. I’ve never been more certain about something over the past few months on this forum. I really think your CCI-like symptoms will improve with styloidectomy. I think your right styloid could be removed too, but your left is definitely priority.
I agree with @TML about the space between the styloid & C1 process, it’s tiny! It would be ideal if you could discuss this with your surgeon & see how high he can remove the styloid to, but if he can’t take any more off, realistically what options do you have? It doesn’t seem possible (from what another Scottish member has said) that you could be referred to England, & options are very limited here too…unless you had plenty of money and could have it done privately with Mr Axon in Cambridge, which I presume isn’t an option?
Wow thank you so much for pointing this out for me. I will phone the secretary tomorrow to see if I can have a chat before surgery to make sure it’s possible to get above the c1 with the TORs. The thing is my radiology report was the most basic report basically saying no masses visible and just reported elongated styloid process on left side, right side withing normal range. When I asked the consultant are my veins and arteries being compressed by it as my symptoms point to this he said no but they obviously are. I can only pray that when he goes in he can see they are compressed and trim it hight about to release. But I will speak to him before surgery and make sure to express I want it above the c1. Ideally I don’t want to travel to England for surgery I want to be close to my family and close to home to get home and recover. But I can thank yous enough for coming in and giving me advice. I will let you know when I get a date.
@Max330 Good plan. Based on the axial slice, your right IJV is slightly compressed bur the styloid is not a culprit (it appears well clear of your right IJV) - so I think your right side could probably stay as is. Your left is definitely beating you up though.
Radiology is notoriously bad at commenting on or being familiar about IJV compression (and even ECA compression) - it’s like they only see our ICAs and if they are good then they think we are good. Really frustrating.
Glad that we could help you with this. Hopefully your surgeon has a plan for you. Please keep us updated!